
At a certain point in every serious lifter’s training career, progress slows down. Not because you’re doing anything wrong. It’s just the reality of approaching your natural ceiling. Your first few years in the gym are relatively straightforward: consistent training, decent food, and you grow. Then the gains start coming in months rather than weeks, and the conversation about what comes next starts.
For a lot of people that conversation eventually includes steroids. But the risks, which include hormonal shutdown, liver stress, cardiovascular impact, the full list of androgenic side effects, are real enough that many lifters want something that sits between natural training and a full steroid cycle. That’s the space SARMs occupy.
Selective androgen receptor modulators were originally developed as pharmaceutical treatments for muscle-wasting diseases, osteoporosis, and hypogonadism. They work by targeting androgen receptors in muscle and bone tissue selectively, rather than flooding every androgen receptor in the body the way steroids do. The result is meaningful anabolic activity with a significantly lower side effect burden.
This guide covers everything you need to make an informed decision: the five most relevant SARMs for bodybuilding, how each one works and who it’s suited for, the best stacks for different goals, PCT guidance, forms and sourcing, and an honest look at what you’re signing up for on the side effect front.
Key Takeaways
- SARMs (Selective Androgen Receptor Modulators) are gaining popularity in the bodybuilding community as a safer alternative to anabolic steroids for building muscle and shedding body fat. 💪
- SARMs have anabolic properties like steroids but with fewer severe side effects, making them a preferred choice for many bodybuilders. ⚖️
- Different SARMs offer specific benefits, such as Testolone RAD 140 for muscle growth and Ostarine MK 2866 for beginners. 🧬
- SARMs come in various forms, including tablets, liquid, and powder, with liquid SARMs being preferred for precise dosage control. 🧪
- While SARMs are generally safer than steroids and prohormones, they may still have side effects, and post-cycle therapy (PCT) is recommended to maintain hormonal balance after a SARM cycle. 🔄

Comparison of the Best SARMs for Bodybuilding
| Feature | RAD-140 | Andarine S4 | YK-11 | Ostarine / MK-2866 | LGD-4033 |
|---|---|---|---|---|---|
| Best for | Lean muscle / Bulking | Fat loss / Cutting | Strength | Beginners | Women / Muscle |
| Dosage | 5–20 mg/day | 25–100 mg/day | 5–30 mg/day | 5–10 mg/day | 5 mg/day |
| Cycle length | 8 weeks | 8 weeks | 4–8 weeks | 8 weeks | 8 weeks |
| Testosterone suppression | Suppressive | Suppressive | Mild | Least suppressive | Suppressive |
| PCT required | ✅️ | ✅️ | ✅️ | Probably | ✅️ |
| Water retention | 🚫 | 🚫 | 🚫 | 🚫 | Slightly |
| Side effects | Minimal | Mild (vision at high dose) | Mild to moderate | Minimal | Minimal |
| For beginners | 🚫 | 🚫 | 🚫 | ✅️ | ✅️ |
How Do SARMs Work?
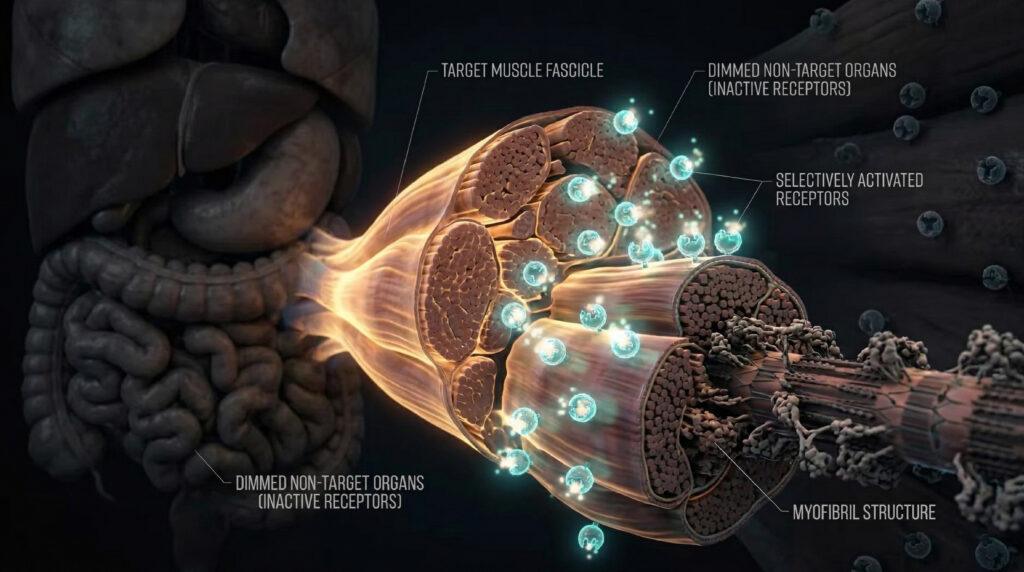
The key difference between SARMs and anabolic steroids comes down to selectivity. Steroids bind to androgen receptors indiscriminately in muscle, liver, prostate, skin, hair follicles, the cardiovascular system. That’s why steroid side effects cover such a wide range of body systems. SARMs are designed to bind primarily to androgen receptors in muscle and bone, which is why their anabolic effects are meaningful while their androgenic side effects are significantly reduced.
When SARMs bind to androgen receptors in muscle tissue, they stimulate the same protein synthesis and muscle fiber development pathways that testosterone activates. They can do this without the same degree of conversion to DHT (which causes hair loss and prostate issues) or estrogen (which causes water retention and gynecomastia).
Some suppression of natural testosterone production still occurs, particularly with more suppressive compounds like RAD-140 and LGD-4033, which is why PCT is necessary for most cycles. But the hormonal disruption is considerably less severe than with a typical steroid cycle.
The 5 Best SARMs for Bodybuilding
1. RAD-140 (Testolone): The Best SARM for Bulking and Lean Muscle
RAD-140 is the compound most serious bulking protocols eventually land on. It has among the highest anabolic-to-androgenic ratio of any SARM currently available, which is why it produces meaningful lean mass gains without the water retention and systemic androgenic effects that make steroids hard to manage.
A 12-week RAD-140 cycle at moderate doses can produce mass gains comparable to a mild testosterone enanthate dose — which is a significant statement for a research compound that doesn’t suppress testosterone to anywhere near the same degree. It also enhances training energy and focus noticeably, which some users credit to its androgenic activity in the CNS.
The one caveat worth flagging: at dosages above 20 mg, some users report a meaningful uptick in aggression. It’s not universal but it’s consistent enough in the community reports that it’s worth being aware of and monitoring, particularly if you’re stacking with other compounds.
Dosage: 5–20 mg/day. 8-week cycle minimum. Follow with PCT.
Best stack: 5 mg RAD-140 + 10 mg MK-677 daily for 8 weeks. Follow with 3 weeks of Clomid PCT.
RAD-140
RAD-140 (Testolone) is a potent Selective Androgen Receptor Modulator (SARM) originally developed to combat muscle wasting and age-related loss of lean tissue. It is designed to selectively bind to androgen receptors in skeletal muscle and bone, producing strong anabolic signaling while minimizing activity in tissues commonly associated with androgenic side effects, such as the prostate and skin.
In research and performance contexts, RAD-140 has demonstrated significant effects on lean muscle gain, strength output, training intensity preservation, and nitrogen retention, making it one of the most sought-after SARMs for recomposition and aggressive muscle-building phases.
Swiss Chems supplies RAD-140 in lab-tested oral formats with third-party purity verification, batch tracking, tamper-resistant packaging, and quality-control standards designed for research consistency and reliability. This focus on sourcing and verification is critical, as underdosed or contaminated RAD-140 remains a known issue in the broader market.
Disclaimer: RAD-140 is a research compound and is not approved by the FDA for human consumption. This content is for educational purposes only and does not constitute medical advice.

RAD-140 Overview
💪 Primary Purpose: Lean mass gain, strength increases, body recomposition
🧪 Form: Capsule
⚗️ Concentration: 10 mg per capsule
📦 Total Content: 60 capsules
💲 Average Price: $89.95
⏱ Typical Research Duration: 6–8 weeks
⚠️ Suppression Risk: Moderate to high
🔗 Common Research Stack: MK-677, YK-11, S4
♂♀ Men/Women: Primarily male research models
Copy Brawn20 for 20% off
- Strong anabolic signaling for lean mass and strength gains
- High oral bioavailability with precise dosing in liquid form
- Effective nitrogen retention and performance support during heavy training mass-building SARM in research settings
- Testosterone suppression is likely with extended use
- Post-cycle recovery protocols are typically required
- Research-only classification; not suitable for beginners
2. Andarine (S4): The Best SARM for Cutting
If the goal is getting lean and dry while holding onto as much muscle as possible, Andarine is the most targeted option available. It works through two mechanisms that are particularly useful on a cut: it suppresses lipoprotein lipase (LPL), a key fat storage enzyme, and it reduces water retention between the skin and muscle — the combination that produces the hard, dry physique most people are chasing in a cutting phase.
S4 doesn’t just allow fat loss; it actively promotes it while maintaining or slightly building lean mass. After a full cycle, muscles typically appear more defined and harder rather than fuller, which makes it the compound of choice when conditioning is the priority over size.
The side effect specific to S4 that you need to know about: at dosages around 50 mg and above, a significant number of users experience a yellow tint to their vision, particularly in low-light conditions. It resolves when the compound is discontinued, but it’s notable enough that many users keep doses below the threshold where it appears.
Dosage: 25–100 mg/day. Most users stay below 50 mg to avoid the vision side effect. 8-week cycle.
Best cutting stack: Andarine 30 mg/day (split across four doses) + Cardarine 20 mg/day (pre-workout) + Ostarine 25 mg/day over 8 weeks.
S4 (Andarine)
S4 (Andarine) is a non-steroidal Selective Androgen Receptor Modulator (SARM) originally developed for research into muscle wasting, osteoporosis, and androgen-deficiency conditions. It works by selectively binding to androgen receptors in skeletal muscle and bone tissue, while minimizing interaction with androgen-sensitive organs.
In laboratory models, Andarine has been studied for its role in lean muscle preservation, fat loss enhancement, recomposition efficiency, and strength output during caloric restriction phases. Its partial agonist behavior makes it a popular research compound for cutting-focused protocols.
SwissChems supplies S4 (Andarine) at 25mg per capsule, 60 capsules per bottle, produced under strict quality control standards with ≥98% purity verification. Each batch is sealed in tamper-proof bottles intended strictly for research use only.
Disclaimer: S4 (Andarine) is a research compound not approved by the FDA for human consumption. This content is for educational purposes only and does not constitute medical advice.

S4 (Andarine) Overview
🔥 Primary Purpose: Cutting, fat loss, lean muscle preservation
🧪 Form: Oral Capsules
📦 Strength: 25mg per capsule
🔢 Bottle Size: 60 capsules
💲 Average Price: $65.95
⏱ Max Research Duration: 6–8 weeks
⚠️ Side Effects: Vision tint changes, headache, suppression risk
🔗 Common Research Stack: Ostarine (MK-2866), Cardarine (GW-501516), SR9009
♂♀ Men/Women: Both (research use only)
Copy Brawn20 for 20% off
- Strong recomposition and cutting research profile
- Preserves lean mass during calorie deficits
- Non-steroidal structure (not an anabolic steroid)
- Oral capsule convenience
- High-purity 25mg dosing format
- Possible vision-related side effects in some research subjects
- Testosterone suppression potential
- Not ideal for pure bulking phases
- Research-only compound
- Not suitable for first-time users
3. YK-11: The Best SARM for Strength
YK-11 is the most aggressive compound on this list and it works through a mechanism that no other SARM replicates: myostatin inhibition. Myostatin is a protein the body produces specifically to limit muscle growth beyond a genetically determined ceiling. YK-11 inhibits it. That ceiling rises, and muscle fiber development accelerates in a way that GH-axis compounds and standard SARMs simply cannot match.
The structural similarities to steroids are more pronounced with YK-11 than with most SARMs, and the side effect profile reflects that — it’s not the compound for beginners and it requires careful cycle management. But for experienced users who have already cycled through milder SARMs and want meaningful strength gains that go beyond what those compounds can produce, YK-11 is the logical next step.
Dosage: 5–30 mg/day. Most protocols use 10–20 mg. 4–8 week cycles due to its potency.
PCT: 4 weeks of Clomid at 20 mg. Begin PCT in the final week of the YK-11 cycle.
4. Ostarine (MK-2866): The Best SARM for Beginners
Ostarine is the right starting point for anyone new to SARMs, and the reason is straightforward: it produces real results — meaningful muscle preservation and modest gains, improved recovery, some fat loss — while having the most forgiving side effect profile in the category. The suppression is the lightest of any SARM, the risk of androgenic side effects is minimal, and the dose range is well-characterised from clinical trial data going back over a decade.
The most useful framing for Ostarine is not as a ‘weak’ SARM but as a compound where the evidence base is broad enough that you actually know what you’re dealing with. That matters when you’re learning how your body responds to androgen receptor modulation before committing to more suppressive compounds.
A typical beginner progression: Ostarine alone on the first cycle, then Ostarine stacked with Cardarine on the second, then a step up to a more potent SARM on the third cycle once you have a clear sense of how your body responds.
Dosage: 5–10 mg/day for beginners; up to 25 mg/day for experienced users. 8-week cycle.
5. Ligandrol (LGD-4033): The Best SARM for Women and Lean Mass
LGD-4033 sits in an interesting position: it’s more suppressive than Ostarine but produces more pronounced lean mass gains, making it the go-to recommendation for women who want a SARM with meaningful anabolic effect at doses where androgenic side effects remain minimal.
For women, the calculus on SARMs is different than for men. The androgenic effect that drives muscle growth in men can cause virilization in women at higher doses or with more androgenic compounds. LGD-4033 at 5 mg/day produces meaningful muscle and strength results for women without the virilization risk that comes with more androgenic options.
For men, LGD-4033 sits as a solid intermediate SARM. It’s more potent than Ostarine for lean mass, less aggressive than RAD-140 or YK-11, with a straightforward dosing protocol.
Dosage: 5 mg/day for women; 5–10 mg/day for men. 8-week cycle. PCT required.
What Are the Different Forms of SARMs?
Liquid SARMs
Liquid is the most common form you’ll encounter for one reason: precise dosing. You can measure exactly 7.5 mg or 12.5 mg or whatever your protocol calls for rather than being locked into a fixed capsule size. A dosing syringe or graduated dropper makes this straightforward, and the compound absorbs quickly.
The biggest downside to this liquid form is taste. Liquid SARMs are generally unpleasant and are best washed down immediately.
There’s also a regulatory logic to liquid form: selling research chemicals in capsule or tablet form implies human consumption more directly. Liquid format creates clearer positioning as a research chemical, which is why most established vendors produce in this form.
Capsule SARMs
Capsules are the most convenient option and have no taste, which matters more than it sounds after a few weeks of liquid SARM protocols. The trade-off is fixed dosing: if the capsule is 10 mg and your protocol calls for 7.5 mg, you either round up or cut capsules, neither of which is ideal. Most experienced users who want precise dose control gravitate toward liquid or powder.
Powder SARMs
Powder is typically the cheapest format per milligram and gives you complete dose flexibility, but it requires a milligram-accurate scale and the patience to measure each dose correctly. The most practical approach is to prepare gel capsules in bulk before a cycle. Get the right dose packed into each capsule before you start rather than measuring loose powder daily. SARMs should never be injected.
Comparing SARMs vs Steroids vs Prohormones
SARMs vs Steroids
The fundamental difference is selectivity. Steroids bind to androgen receptors throughout the body, which is why their side effect profile is so broad. SARMs target androgen receptors in muscle and bone tissue preferentially, producing anabolic effects with significantly less systemic androgenic activity.
In practice: SARMs are less suppressive, don’t convert to estrogen at the same rate, don’t carry the same liver toxicity risk as oral steroids, and don’t produce the same degree of androgenic side effects (hair loss, acne, prostate issues). They are also less potent than steroids at equivalent milligram doses, which is the honest trade-off. If you want the absolute ceiling of anabolic effect, steroids get there. SARMs sit below that ceiling but significantly above natural training.
SARMs vs Prohormones
When anabolic steroids were scheduled in 1990, prohormones emerged as legal alternatives. They work by converting to anabolic hormones through enzymatic processes in the body, effectively serving as hormone precursors. The original prohormones (Epistane, Superdrol) were potent but were banned in 2014. The current generation is considerably weaker.
SARMs are generally more predictable in mechanism, more researched at this point, and produce better results than current-generation prohormones. The suppression and side effect profile is comparable or better, and the quality of available SARMs from reputable vendors is more consistent.
Best SARM Stacks for Bodybuilding
| Stack | Compounds and Dosing | Goal |
|---|---|---|
| GH Maximiser | CJC-1295 DAC + GHRP-6 or GHRP-2 | Maximum GH release for muscle growth and recovery |
| Clean GH Stack | Ipamorelin + CJC-1295 (no DAC) | GH release with fewer hunger and cortisol side effects |
| Bulking Stack | RAD-140 5 mg + MK-677 10 mg daily over 8 weeks + 3-week Clomid PCT | Lean mass gains; comparable to mild testosterone enanthate cycle |
| Cutting Stack | Andarine 30 mg/day (split 4 doses) + Cardarine 20 mg/day (pre-workout) + Ostarine 25 mg/day over 8 weeks | Fat loss, dry hard look, muscle preservation |
| Strength Stack | YK-11 20 mg/day over 8 weeks + 4-week Clomid PCT at 20 mg (begin PCT in final week of cycle) | Maximum strength; myostatin inhibition |
| Beginner Bodybuilder | Ostarine 35 mg + Ligandrol 15 mg over 8 weeks | Lean muscle and fat loss; best introduction to stacking |
NOTE: All stacks require appropriate PCT unless otherwise noted. Start with individual compounds before combining to understand your personal response to each.
Post-Cycle Therapy (PCT)
Even though SARMs are considerably milder than steroids in terms of testosterone suppression, most of them still suppress endogenous testosterone production to a meaningful degree — particularly RAD-140, LGD-4033, and S-23. Running a PCT after your cycle restores natural testosterone levels faster and reduces the effects of suppression: low libido, fatigue, low mood, and reduced strength that can persist for weeks or months without intervention.
The most suppressive SARMs requiring mandatory PCT are RAD-140, LGD-4033, and S-23. Ostarine at low doses may not require PCT, though many users run a light PCT regardless as insurance.
Recommended PCT agents: Clomid (clomiphene) at 20–40 mg/day or Nolvadex (tamoxifen) at 20 mg/day. PCT length: 3–4 weeks. For most SARM cycles, Clomid at 20 mg/day for 3 weeks is standard.
SARM Cycles
Standard SARM cycles run 8 to 12 weeks. For your first cycle, stick to 8 weeks — it gives you a complete picture of how a compound affects you without pushing into the territory where suppression deepens and recovery takes longer. Subsequent cycles can extend to 10 or 12 weeks as you understand your individual response.
Off-cycle time should be at least equal to on-cycle time, inclusive of PCT. If you ran an 8-week cycle and 4 weeks of PCT, wait at least 4 more weeks before your next cycle. This is the minimum — more time off is better for natural testosterone recovery and long-term hormonal health.
SARM Side Effects: What to Actually Expect
The side effect profile of SARMs is genuinely milder than steroids, but ‘milder’ doesn’t mean absent. The most commonly reported side effects across the class include:
- Testosterone suppression: varies significantly by compound. RAD-140 and LGD-4033 are the most suppressive; Ostarine is the least. PCT addresses this but some users experience low testosterone symptoms during the cycle itself.
- Headaches: reported across most SARMs, typically in the first one to two weeks as the body adjusts. Usually transient.
- Mild liver stress: less than oral steroids but not zero, particularly with more potent compounds at higher doses. Standard liver support supplementation (NAC, TUDCA) during a cycle is good practice.
- Vision changes: specific to Andarine S4 at higher doses. A yellow tint to vision, particularly in low light. Resolves on discontinuation.
- Increased aggression: reported with RAD-140 at doses above 20 mg and YK-11. Not universal but worth monitoring.
- Mild acne: less than with steroids but possible, particularly with more androgenic compounds.
The side effects that make steroids genuinely risky — significant cardiovascular impact, severe liver toxicity, permanent hormonal disruption at typical doses — are not associated with SARMs at standard research doses. The risk calculus is meaningfully different, which is why many athletes who want the benefits of androgen receptor activation without the steroid risk profile end up here.
Conclusion
SARMs have brought an exciting new aspect to bodybuilding supplementation as they provide anabolic benefits that are similar to steroids without negative side effects.
In short, SARMs can help to fast-track you on the road to getting big, strong, and ripped.
However, they’re not a magic bullet and you will still need to train intensely and diet diligently.
Combine those two elements with the right SARMs and your bodybuilding results will take off!
Frequently Asked Questions
What is the strongest SARM for muscle growth?
For outright lean mass, RAD-140 (Testolone) produces the most pronounced bulking results of the commonly used SARMs, with a 12-week cycle at moderate doses producing gains comparable to a mild testosterone enanthate protocol. YK-11 produces the most dramatic strength results through its myostatin inhibition mechanism, but it has a more aggressive side effect profile and is not suitable as a first compound. LGD-4033 is a strong alternative for lean mass gains with a slightly more manageable suppression profile than RAD-140
What is the safest SARM for a beginner?
Ostarine (MK-2866) is the correct starting point. It has the lightest suppression profile of any SARM, the longest clinical research history, and a dose range that is well-characterised from over a decade of trial data. The effects are real — meaningful muscle preservation, modest gains, improved recovery — but the risk profile is considerably lower than more potent compounds. Run it alone for a first cycle, understand how your body responds, and move to stacking or more potent SARMs from a position of knowledge rather than guesswork.
Do SARMs require post-cycle therapy?
Most do, yes. The degree of suppression varies significantly by compound — RAD-140, LGD-4033, and S-23 are the most suppressive and require mandatory PCT; Ostarine at low doses is the least suppressive and some users skip PCT at 5–10 mg doses, though a light PCT remains good practice. Clomid at 20 mg/day for 3 weeks is the standard starting point for most SARM PCT protocols. Without PCT after a suppressive cycle, natural testosterone recovery is slower and you’re more likely to spend weeks in a low-testosterone state that erodes the gains you made.
Are SARMs safer than steroids?
Yes, meaningfully so — but the comparison requires context. SARMs are less potent anabolics than steroids, which is part of why they carry a lower risk profile. The selective androgen receptor targeting means they don’t produce the same degree of liver stress, cardiovascular impact, or androgenic side effects (hair loss, prostate issues, acne) that anabolic steroids do at equivalent anabolic effect doses. Testosterone suppression still occurs with most SARMs and requires PCT. Long-term human safety data is more limited for SARMs than for steroids because steroids have been studied and used clinically for longer. They are a meaningfully different risk profile, not a zero-risk alternative.
Can women use SARMs?
Yes, with compound selection being the key consideration. LGD-4033 at 5 mg/day and Ostarine at 5–10 mg/day are the most appropriate options for women — both produce meaningful results at doses where androgenic side effects (virilization — voice deepening, clitoral enlargement, excessive body hair) remain minimal. More androgenic compounds like YK-11, RAD-140 at higher doses, or S-23 carry real virilization risk for women and should generally be avoided. Cardarine (GW-501516) is often included in women’s cycles for fat loss support and doesn’t carry androgenic risk, though it has its own considerations given the carcinogenicity findings in animal studies at extended high doses.












A beginner stack on a 18years-old male increases side effects? Also how much muscle mass can a beginner/intermediate lifter gain in a 8 week cycle? Thanks!