So, you’re on TRT because the stress of daily has taken its toll afters years working that awful job. I get it, but at least we have TRT.
That said, if TRT is supposed to raise your Testosterone, and we know that would leave your Leydig cells inactive… Does TRT make you Infertile? Are you going to be shooting blanks?
Before you (and I both) get ahead of ourselves, most bodybuilders have kids, and they use way more than TRT – so there is some hope. Let’s dig into the science, shall we.
Key Takeaways
- Low testosterone can be challenging in patients who want to become fathers
- Testosterone replacement therapy (TRT) can relieve symptoms of low testosterone, but it can impact fertility and sperm production
- Men of reproductive age with low testosterone should be counseled on the adverse effects of TRT on fertility
- If you are on TRT for low testosterone and want to have children, speak to your doctor and discuss your alternative treatment options that can relieve your symptoms without impacting your ability to have children
What is Testosterone?
Testosterone is a pleiotropic hormone that plays various physiological roles in the development of male genitalia in utero and during puberty.
Classically speaking, testosterone is a hormone associated with masculinity. As an adult, the role of Testosterone is vital in keeping a man fertile, happy, masculine, and even emotionally sound.
What are Normal Testosterone Levels?
In young, healthy men (20 – 30 years old), the normal levels of serum testosterone (400 – 700 ng/dL) are controlled by the feedforward and feedback components of the hypothalamic-pituitary-gonadal axis and are maintained within the normal range of 300–800 ng/dL. [1]
Low Testosterone Levels
Serum testosterone levels decline gradually with age at an approximate rate of 1% per year after the third decade of life. [1]
In 2018, the American Urological Association recommended the use of TRT in patients with total testosterone < 300 ng/dl. [2]
When To Start TRT?
The Endocrine Society and American Urological Association (AUA) recommends treating symptomatic men with low testosterone documented on two morning fasting serum total testosterone concentrations. [3]
Testosterone is used as treatment for males with late onset hypogonadism, a condition in men who experience symptoms caused by a decrease in serum testosterone. [3]
Symptoms associated with low testosterone can include decreased libido, decreased muscle mass, depressed mood and/or erectile dysfunction. [3]
The use of testosterone replacement therapy (TRT) among men over the age of 40 years has increased more than 3-fold over the last decade. [3]
Testosterone and Sperm Production
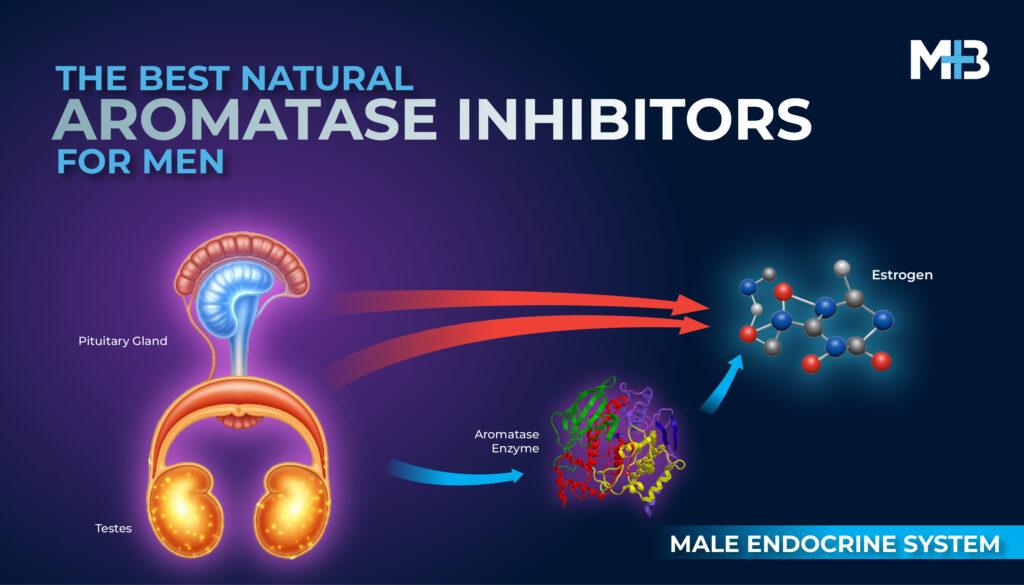
In healthy adult men, testosterone production is precisely regulated by the HPG axis. Higher cortical centers in the brain signal the hypothalamus to secrete gonadotropin-releasing hormone (GnRH) in a pulsatile fashion. [3]
GnRH in turn stimulates the release of LH and FSH from the anterior pituitary which modulates testosterone production from the Leydig cells and spermatogenesis by the Sertoli cells, respectively. [3]
Spermatogenesis is largely dependent on the action of FSH on Sertoli cells coupled with high intra-testicular testosterone concentrations. [3]
Intra-testicular testosterone is required in spermatogenesis for the formation of the blood-testis barrier (BTB). [3]
Testosterone is also required in maintaining connections between Sertoli cells and the haploid spermatid germ cells. [3]
Testosterone aids in this process and increases the efficiency of germ cell attachment to Sertoli cells. Testosterone is also essential for the release of mature spermatozoa from Sertoli cells. [3]
TRT and Fertility
Exogenous testosterone comes in various preparations and each form carries various risks. Along with an increase in hematocrit, a major adverse effect of TRT is the diminished sperm production because of the decreased intra-testicular concentration of testosterone and suppression of the hypothalamic-pituitary-gonadal (HPG) axis. [3]
As testosterone levels increase, negative feedback suppression is exerted on the androgen receptors in the hypothalamic neurons and pituitary gland, thereby inhibiting the release of GnRH, FSH and LH. [3]
The exogenous administration of testosterone suppresses the release of gonadotropins (FSH and LH) to levels below that required for spermatogenesis. [3]
Suppression of follicle stimulating hormone (FSH) release from the pituitary gland impairs sperm production and suppression of luteinizing hormone (LH) release inhibits intra-testicular testosterone production. [3]
The inhibition of LH release by exogenous testosterone leads to the suppression of endogenous testosterone production by the Leydig cells. [3]
The decreased intra-testicular testosterone combined with the suppression of FSH leads to decreased germ cell survival and maturation. [3]
Despite the androgenic effects of testosterone on sexual function, libido and mood; its effect on gonadotropins leads to the inhibition of sperm production. [3]
The Endocrine Society and American Urological Association (AUA)recommend against the use of testosterone for treatment of hypogonadism in men who desire fertility in the next 6 to 12 months. [3]
TRT and Infertility
In 1978, a newly available oral testosterone preparation known as testosterone undecanoate (TU) was investigated as a possible form for male contraception.
The study found that regular testosterone use for 10 to 12 weeks causes suppression of sperm production, and even azoospermia. [7]
Two studies by the World Health Organization (WHO) Task Force on Methods for the Regulation of Male Fertility found an azoospermia rate of 64% to 75% in 6 months with testosterone enanthate.
A sperm concentration of 3 million/mL was used as a threshold for effective suppression of spermatogenesis in this study. [4,8]
In a Chinese study of a monthly intramuscular TU injection, an azoospermia rate of 93% to 98% was achieved after 6 months with 1 million/mL as the criteria for effective suppression in this study. [9]
TRT and Male Fertility: A Guide for Men Planning Parenthood
Consult Your Doctor
Before starting testosterone replacement therapy (TRT), discuss its potential impact on fertility with your doctor.
Understand Fertility Risks
TRT can surprisingly suppress sperm production, despite boosting libido and sexual function.
Discuss Fertility Goals
Talk openly about your current and future plans for children before beginning treatment.
Plan Treatment Timing
Align hypogonadism treatment with your fertility goals to balance symptom relief and family planning.
Blood Work and Semen analyses
Physicians should also educate men already on TRT. There has been an increase in TRT use among men aged 18 to 45 years and more than 20% of these men did not get a baseline testosterone level prior to initiation of TRT. [10]
Some of these men may not know about its effects on fertility and may not have discussed it with their prescribing physician.
This study also showed that less than 2% of men on TRT obtained a baseline semen analysis. In addition to the routine serum total testosterone, LH, and hematocrit prior to starting TRT, every man of reproductive age should have a baseline semen analysis. [10]
The baseline semen analysis will identify men with a decreased baseline sperm count, as a reference value for future semen analyses after TRT use.
How Quickly Does TRT Impact Fertility?
You should know that every body’s response to TRT is different. So, some men may experience quick decline in sperm production while others may experience gradual decline.
It all depends on how well—and fast—the body responds to the additional exogenous testosterone.
Previous study reported that exogenous testosterone can suppress spermatogenesis and lead to azoospermia in 65% of normospermic men within 4 months of use. [4]
Is the Impact of TRT On Fertility Permanent?
In most cases, TRT-induced infertility is not permanent. When TRT is stopped under medical supervision, infertility usually be reversible especially if TRT was only for short-term.
However, for a very small percentage of men, fertility doesn’t return after stopping TRT.
How Long After Stopping TRT Does Your Sperm Count Increase?
Cessation of exogenous testosterone will lead to the reversal of TRT-induced azoospermia in 64% to 84% of men with a median time of about 110 days [4,5].
Azoospermia or severe oligospermia may be seen in these patients, but most men should return to baseline semen analyses in 6 to 9 months after cessation of TRT. [4,5]
All men in these studies recovered to baseline levels after cessation of therapy; however, it took up to 2 years for some men to recover. [4,5]
A 2006 integrated analysis showed that 90% of patients were expected to return to baseline sperm concentration values 12 months after cessation of treatment and 100% after 24 months.
Kohn et al studied spermatogenesis recovery with human chorionic gonadotropin (hCG) and selective estrogen receptor modulators (SERM) in men with infertility associated with TRT use. [6]
In this study, only 30% men were not able to achieve a total motile sperm count of more than 5 million after 12 months in the study. [6]
They found that the failure of recovery is associated with older patients and longer TRT duration. [6]
An older man who was on TRT for a longer time can expect a longer sperm recovery time frame than a younger one who was on TRT for a shorter period of time.
If You Want To Be A Father and You Have Low Testosterone, What Should You Do?
Talk to your doctor. Your doctor will be able to help you determine whether your low testosterone can be normalized by TRT or by alternate treatment option.
For example, there could be a problem with your pituitary gland, in which case pituitary hormone supplementation or another prescription medication could be enough to rectify the low testosterone levels while leaving your sperm production unaffected.
If You’re On TRT and You Want Kids, Should You Stop?
You should never stop TRT on your own. You should never stop TRT suddenly. If you are on TRT and you have a desire to be a father. Talk to your doctor and ask for guidence.
If your doctor determines that stopping TRT is the best course of action because of concerns about TRT and fertility, he may start withdrawing your doses gradually, or consider alternative medications such as clomid to help speed up the increase in sperm count again.
Alternative Options
Human Chorionic Gonadotropin (HCG)
Evidence in a 2015 study of 49 men showed that 3,000 units of hCG subcutaneously every other day is effective in supporting the recovery of spermatogenesis without significant adverse effects.
Adjunctive hCG and Clomiphene
Adjunctive hCG and clomiphene can be used with TRT to maintain testicular size and intra-testicular testosterone concentrations.
Talk To a Specialist
Referral to a reproductive urologist should be considered in a male with low testosterone interested in fertility. TRT clinics and HRT clinics might be able to help you with this.
Preserve Fertility with Sperm Freezing
Low testosterone? Secure your future parenthood by freezing your sperm today.
Sperm freezing involves preserving sperm in liquid nitrogen for future use.
The process is simple:
- Provide a Sample: Produce a semen sample for testing.
- Semen Analysis: Experts assess sperm health and viability under a microscope.
- Freezing: Sperm are frozen at -196ºC to pause biological activity and stored in liquid nitrogen tanks.
Frozen sperm stays viable indefinitely, with no loss in quality or pregnancy potential.
In the future, your stored sperm can be used for intrauterine insemination (IUI) or in-vitro fertilization (IVF).
Act now to safeguard your fertility options.