
You are looking for stopping TRT but you do not know what is going to happen? You are overwhelmed? You are afraid that your lab tests will be back to the baseline before starting TRT? So many options? You are in the right place man!
Stopping TRT is no easy feat, especially if you’ve been on it for a very long time. With so much misinformation on the internet, exactly what happens when you stop TRT?
Key Takeaways
- Before you stop TRT, talk to one of licensed physicians first.
- If you are considering stopping Testosterone replacement therapy because of high costs, side effects, or fertility issues, avoid stopping testosterone replacement “cold turkey,” or you are likely to experience unpleasant symptoms.
- Clomphine citrate and hCG may be good alternative options for you if your healthcare provider agree that they may be beneficial.
- Maintaing a healthy lifestyle is always your first step to a better quality of life.
Testosterone
Testosterone is the primary natural male hormone (produced primarily by the testes), and is responsible for the androgenic (masculinising) and anabolic effects observed during male adolescence and adulthood.
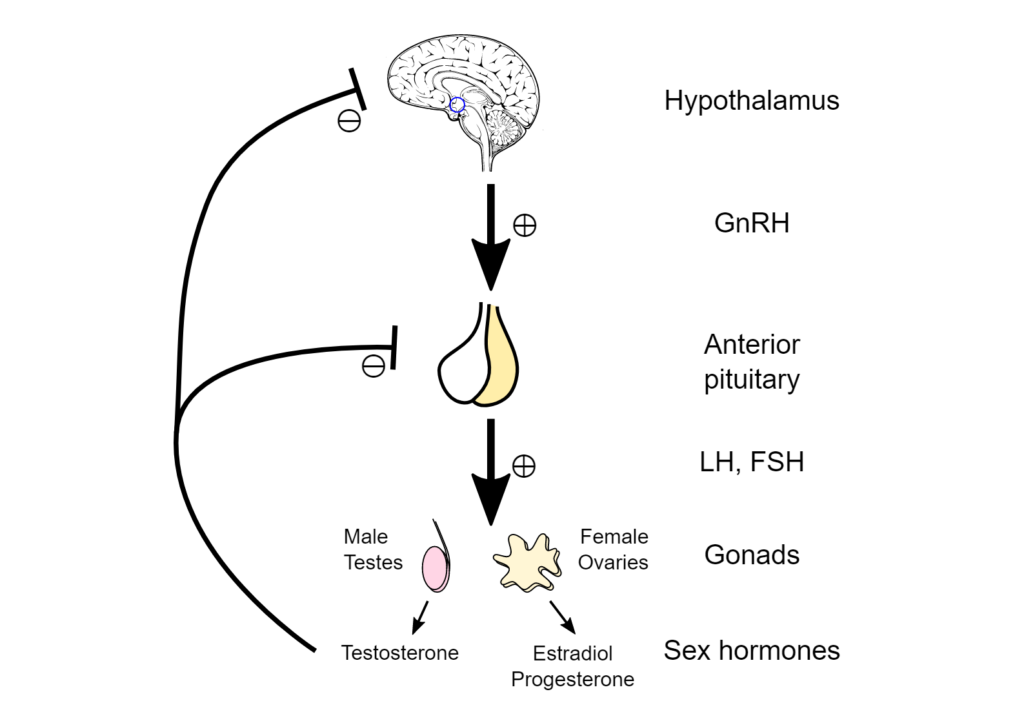
In young, healthy men (20 – 30 years old), the normal levels of serum testosterone (400 – 700 ng/dL) are controlled by the feedforward and feedback components of the hypothalamic-pituitary-gonadal axis and are maintained within the normal range of 300–800 ng/dL. [1]
Low Testosterone Symptoms
Hypogonadism is characterized by low testosterone (T) levels, and is typically treated with testosterone replacement when the etiology is secondary to testicular pathologies. [2]
The diagnosis of adult onset hypogonadism consists of documented low T levels and symptoms indicating testosterone deficiency such as anemia, mood swings, erectile dysfunction, low libido and sexual function, reduced muscle mass and strength, reduced bone mass and osteoporosis, insomnia and a reduced sense of general well-being, forgetfulness, difficulty in concentration, and loss of memory. [2]
Primary hypogonadism is classically defined by low T and elevated gonadotropins. This suggests a dysfunction or failure within the testicle itself. [2]
Causes of primary hypogonadism include testicular infection, infarction, testicular cancer, gonadotoxic medications including chemotherapy, orchiectomy, trauma, and Klinefelter’s syndrome. [2]
Precise diagnosis of these primary testicular disorders is critical since therapies for classic secondary hypogonadism that are aimed at boosting gonadotropins would characteristically not be beneficial in this subgroup. [2]
According to the European Male Aging Study (EMAS), 85% of hypogonadal men are classified as secondary. [3]
Secondary hypogonadism, also referred to as centrally mediated hypogonadism, signifies a disruption in the hormonal axis classically at the hypothalamic and pituitary level. [2]
This results in low T and low or inappropriately low gonadotropin levels. Interestingly, a majority of men diagnosed with secondary hypogonadism have an unknown etiology. [2]
In a study done by Corona et al., it was discovered that 89% of secondary hypogonadal men had an unknown etiology and a majority also carried a diagnosis of metabolic disease which incorporated obesity, type 2 diabetes mellitus or metabolic syndrome. [4]
Testosterone Replacement Therapy
Exogenous testosterone replacement therapy (TRT) is the most commonly studied treatment in adult onset hypogonadism. [2]

Between 2001 and 2011, prescriptions for testosterone replacement therapy among men 40 years of age or older in the US increased more than threefold, from 0.81% in 2001 to 2.91% in 2011. [2]
The use of testosterone replacement has been shown to increase serum testosterone to physiologic levels, improve libido, improve erectile dysfunction, improve overall sexual function, increase energy, improve mood, increase bone mineral density (BMD), decrease body fat mass, and increase lean body muscle mass. [2]
Testosterone Replacement Therapy Complications
Cardiovascular Disease
Data regarding the cardiovascular safety of testosterone replacement therapy have been conflicting and inconclusive. The use of injectable preparations is associated with a greater risk of myocardial infarction and stroke, but not VTE, compared with T gel use.
However, more recent studies have shown that testosterone replacement therapy is not associated with an increased risk of cardiovascular disease.
In general, testosterone treatment is contraindicated in men with severe heart failure as fluid retention may worsen the condition.
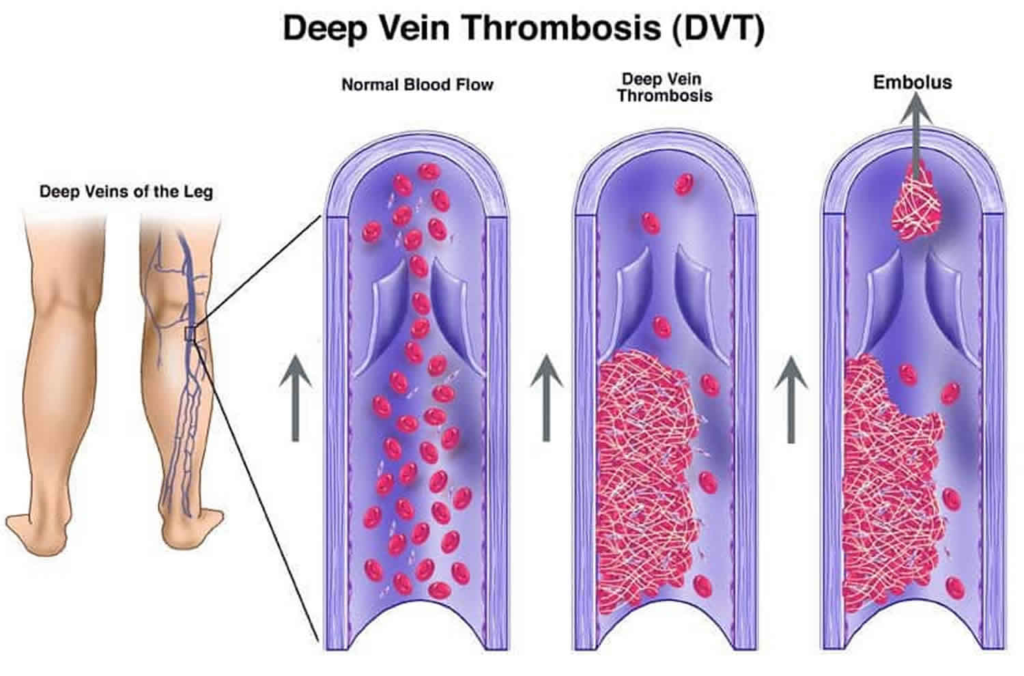
Venous Thromboembolism
The known association between testosterone replacement therapy and erythrocytosis and a report that demonstrated an increased risk of venous thromboembolism in men receiving testosterone therapy, especially in those with underlying thrombophilia, have led the FDA to require adding a general warning to testosterone products about the potential risk for venous blood clots.
Therefore, it is crucial to obtain a careful personal and family history before initiating testosterone therapy.
Erythrocytosis
Erythrocytosis is a common adverse effect of TRT, particularly with testosterone ester injections and in older men. Middle-aged and older men on TRT are nearly four times as likely to have HCT > 50%.
Prostate Cancer
TRT increases prostate volume and PSA. There is unequivocal evidence that TRT can stimulate growth and aggravate symptoms in men with locally advanced or metastatic prostate cancer.
Infertility
The Endocrine Society and American Urological Association (AUA) recommend to stop testosterone replacement therapy for treatment of hypogonadism in men who desire fertility maintain theri sperm production in the next 6 to 12 months.
Exogenous testosterone suppresses LH secretion and thereby decreases the high intratesticular testosterone levels essential for spermatogenesis.
Therefore, hypogonadal men who are being considered for TRT should be told of the suppressive effect of testosterone on spermatogenesis and asked if they desire fertility.
Risks of Stopping TRT Abruptly
Depending on your current dosage, the side effects of stopping “cold turkey” can be pretty harsh, especially if your starting Testosterone levels were extremely low.
- Fatigue
- Weakness
- Decreased muscle mass
- Increased fat
- Thinning hair
- Loss of sex drive
- Depression
- Headaches
- Anxiety
- Insomnia
- Trouble concentrating
How Do You Stop TRT Safely?
Now you are considering ending your TRT, What is next?
- Set an appointment with your doctor.
- Discuss with your medical provider the reasons behind your decision. Whether it’s side effects or costs or fertility and desire to conceive. Just be upfront and honest about your reasons.
- Discuss with your doctor the most suitable plan for you. Gradual withdrawal, and/or finding other alternatives.
What Should You Expect When You Stop TRT?
The short answer is “Back to your baseline before starting TRT”.
You are going to experience the same symptoms you used to have before starting TRT (withdrawal symptoms) such as mood changes, decresed lipido, erectile dysfunction, anxiety, low energy, decreased sex drive, declined sexual performance.
You should also expect your serum testosterone levels to be back to its baseline.
What Is Going To Happen When You Consider Stopping TRT?
Now you are considering stopping testosterone replacement therapy. Talk to your doctor and be honest about what you feel and what you need.
Here are some of the modifications that you may need to apply to your lifestyle in addition to some medical alternatives to discuss with your doctor.
Less Stressful Life
We all know that it may not always be possible to live a stress-free life, but you can do some things to lower your stress levels and therefore boost testosterone levels without the need for exogenous source.
Meditation, yoga, listening to music, etc could be good options for you to maintain a less stressful life.
Sleep Well
Aside from maintaining a healthy weight, sleep quality has been associated with symptoms of low T.
Pastuszak et al. noted a linear relationship between self-reported sleep quality and symptoms of low T as quantified by the Androgen Deficiency in the Aging Male (ADAM) questionnaire.
Workout
A previous study showed that serum testosterone, glycated hemoglobin (A1C), fasting glucose, high‑density lipoproteins (HDL), triglycerides (TG), and waist circumference were significantly improved after 52 weeks of supervised diet and exercise without testosterone treatment.
There is epidemiologic evidence that frequent vigorous exercise is associated with a 30% lower risk of erectile dysfunction.
Moderate physical activity reduces the risk of ED by two‑thirds, and in men with high physical activity, erectile dysfunction. is reduced by over 80%.
The serum testosterone levels of obese men have been reported to be significantly increasing following a 12‑week course of regular aerobic exercise and dietary regulation. They explained that the aerobic exercise and dietary regulation reduced the insulin levels of obese males, leading to increased serum testosterone levels.
Healthy Weight
Low T levels can negatively affect body composition, and as people age, reduced testosterone levels can also cause weight gain. [5]
Studies have shown that both low T and obesity increase the risk of major adverse cardiac events. [5]
Recent preliminary data have shown that low endogenous testosterone levels are associated with lower high-density lipoprotein (HDL) cholesterol and higher low-density lipoprotein cholesterol, triglyceride, and total cholesterol levels. [5]
As such, the AUA recommends counseling men with low testosterone to increase physical activity and maintain their weight within the recommended range to reduce the signs and symptoms of low testosterone and increase serum testosterone levels. [5]
Previous study reported on 68 men participating in a weight-loss diet. Men lost a mean of 10.3–10.8±1.2 kg over the 52-week study period and experienced significant increases in total and free testosterone (P<0.001 and P=0.002, respectively). [5]
Additionally, men with moderate to severe baseline erectile dysfunction had significant increases in the International Index of Erectile Function (IIEF) erectile function domain following weight loss. [5]
More recently, Rigon and colleagues evaluated 29 men with a mean baseline weight of 155.26±25.88 kg preoperatively and 6 months postoperatively following bariatric surgery. [5]
BMI improved to a mean of 37.82±5.94 kg following surgery, with improvements in total testosterone levels from 229.53±96.45 ng/dL to 388.38±160.91 ng/dL (P<0.001). [5]
Alternative Medical Treatment
Anabolic Androgenic Steroids
Anabolic steroids are able to restore testosterone levels in hypogonadal men, thereby increasing fat-free mass, muscle size and strength, and bone density.
Clomiphene Citrate
Clomphine citrate is a selective estrogen receptor modulator. [2]
Originally an agent for female infertility and hyper estrogen states, Clomphine citrate exerts its effect on the hypothalamus and the pituitary gland, acting as an antagonist. [2]
It will increase the endogenous release of gonadotropin-releasing hormones (GnRH), luteinizing hormone (LH) and follicle-stimulating hormone (FSH). [2]
In contrast to pure exogenous testosterone therapy, clomphine citrate offers the advantage of not adversely affecting seminal parameters in symptomatic hypogonadal men seeking to maintain fertility. [2]
The ability of clomphine citrate to improve hormone panels is well supported in the literature. Shabsigh et al. demonstrated that low dose CC (25 mg daily) significantly raised the testosterone level in young men presenting with a testosterone of less than 300 ng/dL. [2]
Subjective symptom relief documented as an improvement in the androgen deficiency in aging males (ADAM) questionnaire has been used as a clinical guide to evaluate symptoms of hypogonadism. [2]
Taylor and Levine observed that men taking clomiphene had a significant improvement in their ADAM score. [9]
In this study, the authors further demonstrated that the improvement in biochemical parameters were similar to that of exogenous testosterone at a much lower cost to the patient. [9]
Tamoxifen
Like clomiphene citrate, tamoxifen has been shown to increase testosterone and gonadotropin levels, and preserve spermatogenesis. [5]
This SERM is an acknowledged alternative treatment option for low testosterone in men. [5]
Tamoxifen has been used to stimulate gonadotropin production, and to treat gynecomastia in the setting of anabolic steroid-induced hypogonadism or hCG treatment. [5]
However, the adverse effects associated with tamoxifen appear to be greater than those associated with clomiphene citrate use, including gastrointestinal distress, venous thromboembolic events, and other cardiovascular outcomes. [5]
As such, tamoxifen is less commonly used for the treatment of low testosterone. [5]
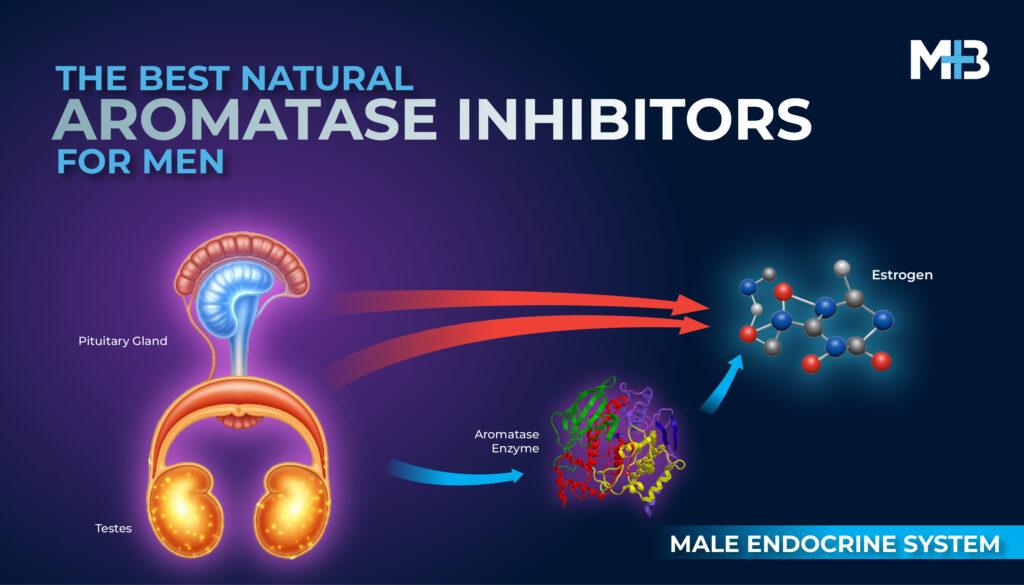
Aromatase inhibitors (AIs)
Estrogen excess has been associated with gynecomastia as well as low gonadotropin and testosterone levels. [2]
Estrogen effects on the gonadotropins and testosterone have led to the evaluation of estrogen as a potential target for treating hypogonadism. [2]
Estradiol is the most potent form of estrogen and its synthesis is a result of the enzymatic activity of aromatase. [2]
Aromatase activity has been found in the gonads, placenta, brain, fat, hair, bone, muscle and vascular tissue. [2]
The conversion of testosterone to estradiol in the gonads has been predicted to be the cause of an increased testosterone/ estradiol (T/E) ratio. [2]
This ratio has been implicated as one of the causes of infertility. Decreased seminal T/E levels have been shown to be a good indicator for identifying the absence of sperm. [2]
Anastrozole and letrozole are examples of third generation non-steroidal AIs originally used in breast cancer therapy that are generally well tolerated. [2]
The lowering of estradiol by AIs has been shown to increase the levels of LH, FSH and testosterone. [2]
In a randomized, double blinded study the researchers demonstrated that clomiphene resulted in significantly higher testosterone levels than anastrozole. [8]
When it comes to subjective clinical improvement the quantitative ADAM scores showed no overall change but there was a small positive trend to improvement in both arms of treatment. [8]
Human Chorionic Gonadotropin (hCG)
Human chorionic gonadotropin is used to promote the endogenous production of testosterone without compromising spermatogenesis. [6]
It is FDA approved alternative therapy for males with low testosterone and wish to preserve their fertility. [6]
It is also efficacious in inducing spermatogenesis. It is even effective in helping with the recovery of spermatogenesis in men who were on testosterone replacement therapy. [7]
Clinicians generally agree on using 2,000 IU of hCG administered subcutaneously 3 times per week as defined by the 2002 American Association of Clinical Endocrinologists guidelines. [7]
HCG may help maintain natural testosterone levels and keep your testicles in good health, both of which are important for maintaining natural testosterone production and fertility, respectively.












I have been on trt for approx 11 months and are experiencing severe headaches exacerbated by coughing, I cut down my 1 ml oinjections to 1/2 2x weekly but headaches were still there, had a nasal ct scan and brain mri all was inconclusive, have stopped trt completly for 3 weeks still having headaches,
I have been on TRT for 11 months, just quitting now.
It’s going to be tough .