Picture a teen who loved sports but now struggles to climb stairs. The legs grow heavy, and the shoulders tire quickly after even simple tasks. Over months the weakness grows. This is how muscular dystrophy can enter a family’s life.
Muscular dystrophy is a group of genetic diseases that cause progressive muscle weakness. The disease affects skeletal muscles first. Some forms also involve the heart muscle and breathing muscles. Most types progress slowly. A few move fast. Early diagnosis and the right care plan help people keep functioning for longer.
This guide breaks down the main muscular dystrophy types. You will learn symptoms, age of onset, muscles involved, inheritance patterns, tests, and care.
Key Takeaways
- Muscular dystrophy includes many disorders with different genes and patterns, not a single disease. 🧬
- The main symptom is progressive muscle weakness that affects daily tasks like walking and lifting. 💪
- Early diagnosis guides care for the heart, lungs, and mobility which protects quality of life. 🩺
- Most forms have no cure yet, but exercise guidance, respiratory care, and new drugs improve outcomes. 🌟
- Genetic counseling helps families understand risks and plan for the future. 👨👩👧👦

How Muscular Dystrophy Damages Muscle
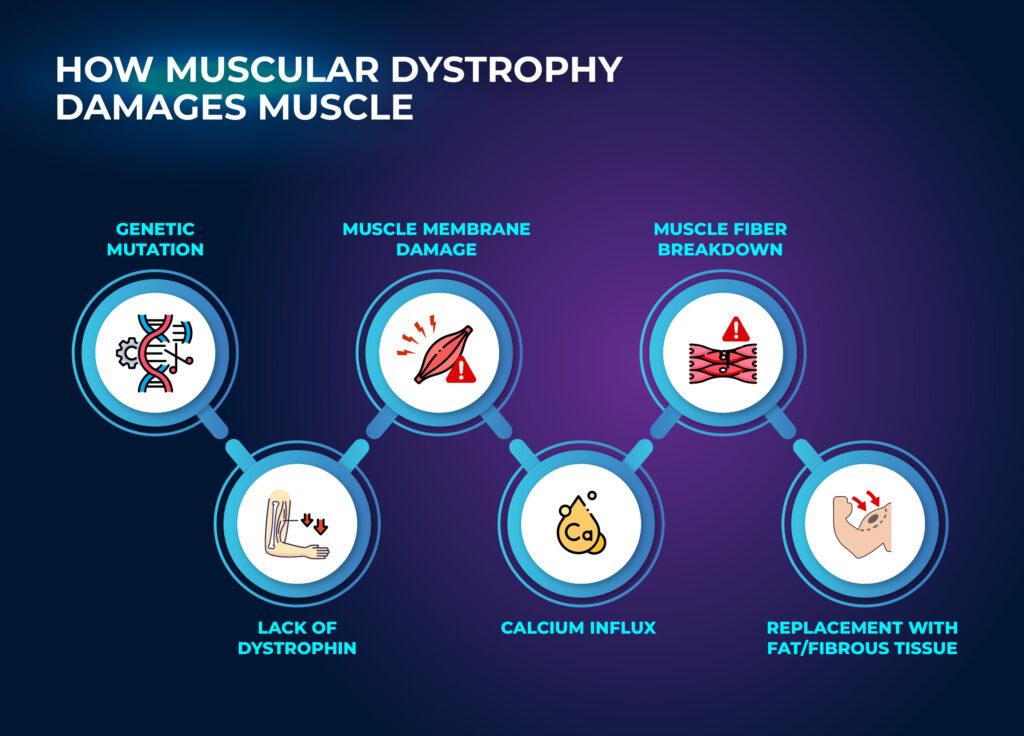
Muscle fibers rely on proteins that hold cells together and help them contract. Gene mutations change these proteins. The result is fragile muscle fibers that break down during normal use. Inflammation and scar tissue follow. Over time the muscle thins and weakens.
Different genes explain the different muscular dystrophy types. Dystrophin loss drives Duchenne and Becker muscular dystrophy. Sarcoglycan, calpain, dysferlin, and lamin A/C defects drive many limb girdle muscular dystrophy forms. FSHD comes from abnormal activation of the DUX4 gene. Myotonic dystrophy comes from DNA repeat expansions that disrupt many cell functions.
Types of Muscular Dystrophy
Below is a quick comparison. Details for each type follow.
| Type | Typical onset | Muscles involved first | Inheritance | Progression | Life expectancy |
| Duchenne muscular dystrophy – DMD | Early childhood | Hips, thighs, shoulders, calves | X chromosome linked | Rapid | Shortened without modern care |
| Becker muscular dystrophy | Late childhood to young adulthood | Hips, thighs, calves | X chromosome linked | Slower than DMD | Near normal in some patients |
| Limb girdle muscular dystrophy – LGMD | Childhood to adulthood | Upper legs and upper arms around hips and shoulders | Autosomal dominant or recessive | Variable | Often near normal to mildly shortened |
| Facioscapulohumeral muscular dystrophy -FSHD | Teens to early adulthood | Face, shoulder blades, upper arms | Autosomal dominant | Slow with flare periods | Often normal life span |
| Myotonic dystrophy – DM1 DM2 | Teens to adulthood. Congenital form at birth in DM1 | Hands, face, neck. Trouble relaxing muscles | Autosomal dominant | Slow but multisystem | Reduced in severe forms |
| Emery Dreifuss muscular dystrophy – EDMD | Childhood to early adulthood | Lower legs, upper arms. Early joint contractures | X linked or autosomal | Slow. Heart rhythm risk | Depends on heart rhythm care |
| Oculopharyngeal muscular dystrophy – OPMD | Mid to late adulthood | Eyelids and throat muscles | Autosomal dominant or recessive | Slow | Near normal with swallow care |
| Distal muscular dystrophy | Early adulthood to later life | Lower legs and lower arms first | Usually autosomal dominant | Slow | Often normal life span |
| Congenital muscular dystrophy – CMD | Birth or early infancy | Generalized weakness. May include breathing and joints | Autosomal recessive most often | Variable | Depends on subtype and care |
Duchenne Muscular Dystrophy
Duchenne muscular dystrophy is the most common form in boys. It usually appears between ages two and five. The main symptom is progressive muscle weakness in the upper legs and hips. Children have frequent falls. They struggle with running and climbing stairs. Calf muscles may look large but feel weak.
This disease affects boys because the gene sits on the X chromosome. Boys have one X chromosome so a single mutation can cause disease. Girls can carry the mutation and rarely show symptoms. The missing protein is dystrophin. Without dystrophin the muscle fiber membrane tears during normal activity.
Other symptoms appear as the disease progresses. The shoulders weaken. A curved spine may form. Heart problems and breathing problems develop in the teen years. Some boys have learning or attention issues. Early care with steroids, heart medicines, and respiratory care improves function and extends life.
Becker Muscular Dystrophy
Becker muscular dystrophy is a milder form related to dystrophin. The gene mutation allows the protein to be present but shorter or reduced. Symptoms start later. Young adults often notice fatigue in the legs during sports. The disease affects the same muscles as Duchenne but progresses more slowly. Many people with Becker maintain walking into adulthood. Heart muscle involvement is common and needs regular checks.
Limb Girdle Muscular Dystrophy
Limb girdle muscular dystrophy refers to a group of many subtypes. The disease affects the muscles around the hips and shoulders first. People notice trouble rising from a seated position. They have difficulty climbing stairs and lifting overhead. Males and females are affected equally because the inheritance is autosomal. Some forms are recessive. Others are dominant.
The pace of weakness depends on the gene. Sarcoglycan, calpain, dysferlin, and other protein defects can lead to similar symptoms. Calf enlargement is common in some subtypes. Heart or breathing muscle can be involved in selected forms. Genetic testing is important to define the exact type because it guides monitoring and family counseling.
Facioscapulohumeral Muscular Dystrophy
Facioscapulohumeral muscular dystrophy usually begins in the teenage years or early adulthood. It weakens facial muscles first. People may struggle to whistle or close their eyes tightly. The shoulder blades wing out and the upper arms tire easily. Leg involvement can appear later and cause difficulty walking long distances.
FSHD is often autosomal dominant. One affected parent can pass it to a child. The condition progresses slowly. Many people keep normal life spans. Pain in the shoulders and lower back can be significant. Exercise plans focus on posture, scapular stability, and energy conservation.
Myotonic Dystrophy
Myotonic dystrophy has two major forms called type 1 and type 2. Type 1 can also present as a severe congenital form at birth. The key feature is myotonia which means the muscle does not relax right away after a contraction. People have trouble releasing a grip. The face and neck may appear thin. Weakness often starts in the hands and feet.
Myotonic dystrophy affects more than muscles. It can involve the heart rhythm, cataracts, thyroid, and blood sugar. Daytime sleepiness is common. Because the disease affects many organs, care requires a coordinated healthcare team. Genetic counseling is important because the condition is autosomal dominant.
Emery Dreifuss Muscular Dystrophy
Emery Dreifuss muscular dystrophy causes early joint stiffness called contractures. The elbows, ankles, and neck may lose range of motion in childhood or early adulthood. Muscle weakness often starts in the lower legs and upper arms. The most serious risk is heart rhythm problems. People need regular heart rhythm checks and early treatment when needed.
EDMD can be X linked or autosomal. Gene mutations include EMD, FHL1, and LMNA. Families may call it Dreifuss muscular dystrophy or EDMD. The progression is slower than Duchenne. With careful heart care, many people remain active and independent.
Oculopharyngeal Muscular Dystrophy
Oculopharyngeal muscular dystrophy begins in midlife. The first signs are droopy eyelids and trouble swallowing. People may clear the throat often. Meals take longer. Food may feel stuck. The voice can sound nasal. Limb weakness can develop later but is often mild.
OPMD is more common in some regions and families. The inheritance can be dominant or recessive. Swallow studies and speech therapy help prevent choking. Minor eyelid surgery can improve vision when droop blocks the eyes. Most people have a normal life span.
Distal Muscular Dystrophy
Distal muscular dystrophy affects the hands, forearms, lower legs, and feet first. Grip strength falls. Ankle weakness leads to tripping. Symptoms often begin in early to late adulthood. The pace of progression is slow. Many people keep a normal life span.
Several genes can cause distal forms. The pattern may be dominant in a family. Heart and breathing muscles are usually spared but should be checked. Focus on joint protection and safe training helps preserve function.
Congenital Muscular Dystrophy
Congenital muscular dystrophy presents at birth or in the first months of life. Babies feel floppy and have poor head control. Feeding can be difficult. Some forms affect the eyes and brain. Others cause tight joints or a very rigid spine.
CMD includes many subtypes and most are autosomal recessive. The care plan focuses on breathing support, nutrition, mobility devices, and early therapy. Some forms have severe disability. Others allow walking with minor disabilities. The range is wide, so families need clear genetic results and a personalized plan.
Symptoms You Might Notice Day to Day
- Frequent falls and difficulty walking long distances
- Trouble climbing stairs or rising from a seated position
- Shoulder fatigue with reaching overhead or carrying
- Weak grip and hand cramps in myotonic or distal forms
- Droopy eyelids and trouble swallowing in oculopharyngeal forms
- Curved spine and tight joints in selected types
- Shortness of breath with exertion in advanced disease
How Is Muscular Dystrophy Diagnosed
Getting muscular dystrophy diagnosed early changes the path. Doctors start with a careful history that looks for age at first symptoms, frequent falls, late walking, or trouble climbing stairs in early childhood. They ask about relatives with similar symptoms or early heart problems. The physical exam maps which muscles are weak, such as upper legs, upper arms, lower legs, or facial muscles.
Common tests:
- Creatine kinase blood test. Very high levels suggest active muscle fiber damage.
- Genetic testing. Modern panels find gene mutations for various subtypes.
- Electromyography. Shows electrical patterns that support a muscle disease instead of a nerve disease.
- Muscle biopsy. Used when genes are unclear. It shows loss of key proteins like dystrophin or sarcoglycans.
- Heart tests. ECG and echocardiogram look for rhythm and muscle changes, especially in Duchenne, Becker, myotonic dystrophy, and EDMD.
- Lung tests. Simple measures track diaphragm strength and guide respiratory care.
Ask your healthcare team about national institute funded resources and registries. These programs support access to trials and standards of care.
Treatment and Day to Day Management
There is no single cure yet. Care aims to slow weakness, protect the heart and lungs, and keep independence. Some newer therapies target specific gene mutations, including exon skipping and microdystrophin approaches for Duchenne muscular dystrophy.
Core pieces of care:
- A neuromuscular specialist to lead the plan
- Physical therapy for flexibility and safe strength work
- Occupational therapy for tools that make daily tasks easier
- Respiratory care with cough training and support devices when needed
- Cardiology care for rhythm and heart muscle checks
- Nutrition support to maintain a healthy weight
- Mental health support for the person and the family
Medications and devices:
- Corticosteroids can slow muscle loss in Duchenne
- Heart medicines support function in Duchenne and Becker
- Pacemakers or defibrillators may be lifesaving in EDMD
- Noninvasive ventilation supports breathing during sleep in several forms
- Orthotics and lightweight wheelchairs reduce energy cost and prevent falls
Exercise guidance:
Light to moderate activity helps preserve function. Avoid heavy eccentric loading that causes muscle soreness and pain the next day. Pool work and cycling reduce joint stress. Rest between sessions. Track fatigue and adjust volume. A physical therapist can design a plan that fits your current strength.
Limb Girdle Focus: What To Watch For
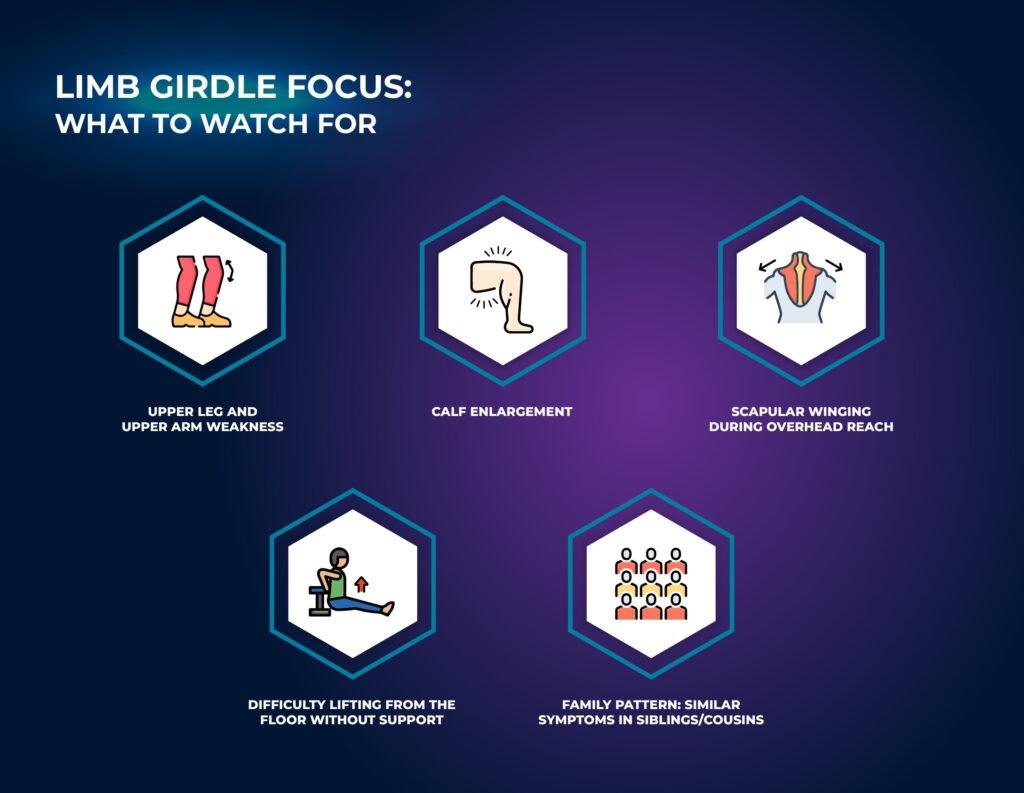
Because limb girdle muscular dystrophy has many genes, watch for patterns.
- Weakness in the upper legs and upper arms
- Calf enlargement in some subtypes
- Shoulder blades that wing with overhead reach
- Trouble lifting from the floor without support
- Similar symptoms in siblings or cousins
Genetic results name the exact subtype which shapes monitoring. For example, dysferlin related disease may progress slowly but affect lower legs. Sarcoglycan defects can involve the heart muscle more often.
Life Expectancy and Quality of Life
Life expectancy varies by type and by care access. Duchenne muscular dystrophy DMD historically reduced life to the late teens. With modern steroids, heart care, and respiratory care, many now live into their late 20s and 30s. Some reach their 40s.
Becker muscular dystrophy can allow a normal life span with careful heart monitoring. FSHD, distal muscular dystrophy, and oculopharyngeal muscular dystrophy often allow normal life spans. Limb girdle muscular dystrophy and myotonic dystrophy are variable. Severe early onset forms shorten life. Adult onset forms often have milder symptoms and near normal life spans.
Quality of life improves with early planning. Home and school accommodations, timely mobility aids, and airway support reduce crises. A strong healthcare team and a clear exercise plan reduce hospital stays. Families who learn about their specific type feel more in control.
Everyday tips
- Keep vaccinations current to prevent lung infections
- Plan daily tasks to avoid fatigue peaks
- Use seating and transfer aids early to prevent falls
- Ask about sleep studies if morning headaches or daytime sleepiness appear
- Track mood and energy. Ask for support when stress rises
Muscles Involved By Region
- Upper legs and hips in Duchenne, Becker, and many limb girdle forms
- Upper arms and shoulders in FSHD, limb girdle, and EDMD
- Lower legs in distal forms and EDMD
- Throat muscles in oculopharyngeal muscular dystrophy
- Face muscles in FSHD and myotonic dystrophy
Red Flags That Need Fast Care
- New chest pain, palpitations, or fainting
- Worsening morning headaches or daytime sleepiness which suggests night breathing problems
- Repeated choking or weight loss from trouble swallowing
- Sudden change in walking or frequent falls with injuries
How Muscular Dystrophy Affects Boys, Girls, Men, and Women
Duchenne and Becker are X linked. They affect boys most. Some girls and women who carry the gene can have mild weakness or heart issues. Limb girdle, FSHD, myotonic dystrophy, distal, and most congenital forms affect men and women equally. In autosomal dominant diseases one affected parent can pass the condition to a child of any sex. Genetic counseling explains risks for each family.
Final Reps: What To Remember About Muscular Dystrophy Types
Muscular dystrophy types share one core driver. A genetic mutation weakens muscle fibers and leads to progressive muscle weakness. The disease affects muscles in the upper legs, upper arms, lower legs, and sometimes the heart muscle and throat muscles.
Knowing the exact type, such as Duchenne muscular dystrophy, Becker muscular dystrophy, limb girdle muscular dystrophy, facioscapulohumeral muscular dystrophy, myotonic dystrophy, oculopharyngeal muscular dystrophy, distal muscular dystrophy, or Emery Dreifuss muscular dystrophy, guides care and expectations for life expectancy.
Act early and build a strong healthcare team. Use genetic testing to confirm the diagnosis. Plan safe activity, respiratory care, and heart screening. Watch for red flags like trouble swallowing, frequent falls, or new palpitations. With the right plan many people keep independence, work or study, and live meaningful lives even as the disease progresses slowly.
Frequently Asked Questions (FAQs)
What is the most common type of muscular dystrophy?
Duchenne muscular dystrophy is the most common form in children. Myotonic dystrophy is the most common adult form.
How is muscular dystrophy diagnosed?
Doctors use a history, exam, creatine kinase, genetic testing, and sometimes a muscle biopsy. Heart and lung tests look for silent involvement.
Can someone with muscular dystrophy exercise?
Yes with guidance. Choose low impact movements. Stop if you feel muscle pain that lasts into the next day. Focus on posture, flexibility, and safe strength.
Do all forms affect the heart?
No. Some forms involve the heart muscle more often. Examples are Duchenne, Becker, myotonic dystrophy, and EDMD. Regular screening finds problems early.
What is the role of nutrition?
A balanced diet supports energy and weight control. Soft or blended foods help in oculopharyngeal muscular dystrophy. A dietitian can guide safe calorie and protein targets.