I’ve run tesamorelin in two separate protocols over the past couple years, and the single biggest mistake I see people making is overdosing this peptide. The standard tesamorelin dosage per day is 2mg administered via subcutaneous injection, typically taken before bed or first thing in the morning on an empty stomach.
That’s the FDA-approved dose. But the bodybuilding and anti-aging communities have been experimenting with lower amounts…and honestly, from what I’ve seen, plenty of people get solid results at 1mg per day.
Tesamorelin is one of those peptides that actually made it through the FDA approval process, which is rare in this space. It was originally developed for HIV-associated lipodystrophy, which refers to that stubborn visceral fat accumulation that’s notoriously hard to target. But its ability to stimulate natural growth hormone production has made it popular well beyond that original use case.
Key Takeaways
- Tesamorelin is a GHRH analog that boosts natural GH and IGF-1 levels for targeted metabolic effects. 🔬
- Clinical trials show reduced visceral fat, better body composition, and improved lipid profiles. 💪
- FDA-approved for HIV-related lipodystrophy, with growing off-label use in bodybuilding and recovery. ✅
- Standard dosing is 1 mg daily (5 days on, 2 off) with proper site rotation and clean injection practices. 💉
- Side effects are generally mild, but medical guidance ensures safe and effective use. ⚠️

What Is Tesamorelin?
Tesamorelin is a synthetic growth hormone-releasing hormone (GHRH) analog consisting of 44 amino acids with a trans-3-hexenoic acid modification at the tyrosine residue.
Sold under the brand name Egrifta, tesamorelin was approved by the FDA in 2010 specifically for reducing excess abdominal fat in HIV-positive patients with lipodystrophy. It’s not synthetic HGH — that’s a common misconception. Instead, it works upstream by telling your pituitary gland to do its job and release more growth hormone naturally. Big difference.
The reason this peptide became so popular outside its original indication is simple: it selectively targets visceral adipose tissue. That’s the deep belly fat wrapped around your organs that’s both cosmetically frustrating and metabolically dangerous. In the landmark study published in the New England Journal of Medicine (2007), tesamorelin reduced trunk fat by approximately 15% over 26 weeks compared to placebo. Most GH-related compounds don’t show that kind of targeted fat reduction in clinical settings.
I’d say about 70% of the people I talk to who are using tesamorelin are doing it for body composition — not because they’re HIV-positive. The anti-aging crowd has latched onto it too, thanks to its ability to boost IGF-1 levels without the side effect profile of exogenous HGH.
How Does Tesamorelin Work?
Most guides will tell you tesamorelin “stimulates the growth hormone.” That’s not wrong, but it undersells the mechanism.
Tesamorelin binds to GHRH receptors on somatotroph cells in the anterior pituitary gland. Once bound, it triggers a signaling cascade through the cAMP/protein kinase A pathway, which causes these cells to synthesize and release stored growth hormone into circulation. The key here is that your body’s natural feedback loops remain intact. When GH levels get high enough, somatostatin kicks in to pump the brakes. This pulsatile release pattern is what makes tesamorelin fundamentally different from injecting exogenous HGH, where you’re essentially bypassing that entire regulatory system.
The downstream effects are what people actually care about. Elevated GH stimulates hepatic IGF-1 production, which drives many of the anabolic and lipolytic effects — fat mobilization, protein synthesis, connective tissue repair. The pivotal Phase III trial published in the New England Journal of Medicine (Falutz et al., 2007) found that tesamorelin increased IGF-1 levels by approximately 81% over baseline after 26 weeks, compared to a 5% decrease in the placebo group (p<0.001). That’s a meaningful, proportional rise without pushing levels into supraphysiological territory for most users.
There’s also emerging evidence that tesamorelin may have direct effects on hepatic fat. A study published in Hepatology (2019) found it reduced liver fat by about 37% in HIV patients with nonalcoholic fatty liver disease. Whether that translates to the general population is still being studied, but it’s promising data.
Tesamorelin Dosage By Goal
Fat Loss and Body Recomposition
This is why most people are here. For visceral fat reduction, the clinical evidence supports 2mg daily for a minimum of 12 weeks. The pivotal Phase III trials (Falutz et al., 2007 and 2010) used this exact protocol and showed a mean reduction in trunk fat of 15-18%. Results tend to plateau around the 26-week mark, which is why most protocols don’t extend much beyond that without a break.
If you’re stacking tesamorelin with a caloric deficit and consistent training, you’ll likely notice abdominal fat changes around weeks 6-8. I didn’t see dramatic visual changes until about week 10 on my first run, but bloodwork showed elevated IGF-1 by week 4.
Anti-Aging and General Wellness
The anti-aging crowd tends to run lower doses. 1mg per day is common here, and honestly, that’s probably sufficient if your primary goals are improved sleep quality, skin elasticity, and general recovery. You won’t get the same degree of visceral fat reduction, but your wallet won’t take as much of a hit either. Some clinics prescribe tesamorelin at this dose alongside other longevity-focused protocols.
Muscle Gain Support
Let me be blunt here — tesamorelin isn’t going to pack on slabs of muscle the way anabolics do. That’s not what it’s for. The GH elevation you get from 2mg daily is modest compared to running exogenous HGH at 4-6 IU. That said, the indirect benefits — better recovery, improved sleep, enhanced nutrient partitioning, reduced body fat — create a better environment for gains when you’re training hard. Think of it as a supporting compound, not a primary driver.
Most bodybuilders running tesamorelin for lean mass purposes stick to 2mg per day and stack it with something like ipamorelin to amplify the GH pulse. More on stacking below.
Liver Fat Reduction
This one’s underrated. The 2019 Hepatology study I mentioned earlier used 2mg daily for 12 months and saw a 37% reduction in hepatic fat fraction. If you’re someone who’s been on-cycle with orals and you’re concerned about liver health (and you should be if you’ve run oral anabolic steroids), tesamorelin is worth a serious look during your off-cycle recovery period.
How to Use Tesamorelin
Tesamorelin comes as a lyophilized (freeze-dried) powder that you’ll need to reconstitute before injecting. If you’ve used any peptide before — BPC-157, TB-500, whatever — the process is identical.
- Reconstitute with bacteriostatic water (BAC water). For a 2mg vial, I typically add 1mL of BAC water. This gives you a clean 2mg/mL concentration, making dosing simple.
- Swirl gently — never shake. Peptides are fragile. Shaking can denature the protein structure and tank your product’s potency.
- Draw your dose using an insulin syringe. At 2mg/mL concentration, you’d draw the full 1mL (100 units on an insulin syringe) for a 2mg dose, or 0.5mL (50 units) for a 1mg dose.
- Inject subcutaneously. Common sites are the lower abdomen (rotating injection spots), the fatty area around your love handles, or your thigh. Pinch the skin, insert at a 45-degree angle, inject slowly.
- Store reconstituted tesamorelin in the refrigerator. Use within 20-28 days once mixed.
One quick note on timing — inject when your stomach has been empty for at least 2 hours. Eating within 30 minutes of your shot can significantly blunt the GH response. Most people do it right before bed or first thing in the morning. I prefer the bedtime protocol because GH naturally peaks during deep sleep anyway, so you’re amplifying what your body already wants to do.
Cycle Length and Protocol
So how long should you actually run this? The clinical trials ran 26 weeks (about 6 months), and that’s generally considered the sweet spot for maximum benefit. After 26 weeks, GH response can start to diminish slightly as your pituitary adjusts.
Here’s what I’d recommend based on experience and the available data:
| Protocol | Duration | Notes |
| Standard Run | 12-26 weeks on, 4-8 weeks off | Most common approach, mirrors clinical trial design |
| Extended Run | 26+ weeks continuous | Used in some clinical settings; monitor IGF-1 levels |
| Conservative Cycle | 8-12 weeks on, 4 weeks off | Good for budget-conscious users or first-timers |
There’s no hard evidence that you need to cycle off tesamorelin the way you’d cycle off, say, SARMs. It doesn’t cause pituitary suppression in the same way. But anecdotally, taking periodic breaks seems to maintain sensitivity to the compound. I usually do 16 weeks on, 4 weeks off, then reassess based on bloodwork.
One thing that’s different from exogenous HGH — you don’t need to taper. Just stop. Your body’s natural GH production should resume its baseline pattern within a few days to a couple weeks.
Stacking Options for Tesamorelin
Stacking Options
Tesamorelin pairs extremely well with other GH secretagogues. The most popular stack I’ve seen (and used) is tesamorelin with ipamorelin. The logic is straightforward: tesamorelin stimulates GH release via the GHRH pathway, while ipamorelin hits the ghrelin/GHS-R1a pathway. Two different mechanisms, synergistic effect. You’re essentially pressing the gas pedal from two different angles.
Common stacks include:
- Tesamorelin + Ipamorelin: 2mg tesa + 200-300mcg ipamorelin before bed. The gold standard GH peptide stack.
- Tesamorelin + CJC-1295 (no DAC): 2mg tesa + 100mcg CJC-1295. Adds sustained GHRH activity. Some people find this redundant since tesamorelin already hits the GHRH receptor, but the pharmacokinetics differ.
- Tesamorelin + BPC-157: Useful if you’re recovering from an injury. BPC-157 at 250-500mcg twice daily handles the tissue repair side while tesamorelin provides systemic GH support. If you’re curious about BPC, we’ve got a solid breakdown of peptide protocols and results.
I wouldn’t stack tesamorelin with exogenous HGH. That’s redundant and potentially counterproductive — exogenous GH suppresses your pituitary’s natural output, which is the exact mechanism tesamorelin relies on.
Tesamorelin Experiences
As I started to read personal experiences of people using Tesamorelin on a credible website, people had mixed opinions.
Here are some of the reviews I could find:
“Just finishing 2 months on Egrifta. 1st month is not remarkable but at the 6 weeks mark, I’m noticing a change. It seems as if the visceral fat has reduced and moving to sub-q fat. I’ve maintained the same diet, medication, and workout schedule. Just about 7 lbs. weight loss but not sure it’s the Egrifta. Will check in at the 3-month mark.”
-Brainsbelly
“I have been on Egrifta for 14 months. It took 6 months before I noticed much. I am now pleased with the results and will continue to use the product.”
-Jack
“Body aches, nausea, but it is working. Not actual weight, but reducing belly fat”
-Steve
“I have been administering Egrifta now for 2 1/2 months, with absolutely no reduction of abdominal fat. I am a thin person with my abdominal fat causing me to be unable to close the buttons and zippers of my clothing. Then I heard of Egrifta thinking it was the answer. Wrong! No results, just a painful irritated, scar tissue in my abdomen now.”
-Mad
“I began the Egrifta Injection at 2 ml per day. I began feeling the fat soften within the first week. I began the medication weighing 226.2 lbs and in less than 6 months I weighed 198.2 lbs. Then my GH1 level shot up and within 2 weeks every bit of the weight I had lost all returned plus. By the way, once you begin taking this cover-up drug, you’re on it the rest of your life, or the fat returns.”
-Anonymous
Tesamorelin Side Effects
Tesamorelin is genuinely well-tolerated. Not just compared to anabolics (that’s a low bar), but compared to most peptides in general.
The most common side effects from the clinical trials were:
- Injection site reactions: redness, itching, swelling. This happened in about 24% of subjects in the Phase III trials. Usually resolves within minutes to hours.
- Joint pain and stiffness: classic GH-related side effect. Happens because elevated GH causes fluid retention in joint spaces. Typically mild.
- Peripheral edema: mild water retention, especially in the hands and feet. If you’re seeing significant bloat, your dose might be too high.
- Paresthesia: tingling or numbness, usually in extremities. Reported in roughly 5% of trial participants.
Rare but documented: elevated blood glucose. GH is a counter-regulatory hormone to insulin, so prolonged use at higher doses can impair glucose tolerance. If you’re pre-diabetic or insulin resistant, monitor your fasting glucose and HbA1c while running tesamorelin. This isn’t something to brush off.
Also — and this applies to all GH-elevating compounds — there’s a theoretical concern about stimulating growth in existing malignancies. If you have any active cancer or a history of certain cancers, tesamorelin is contraindicated. Not negotiable.
Tesamorelin
Tesamorelin (Egrifta) is a synthetic analog of Growth Hormone–Releasing Hormone (GHRH), studied for its ability to modulate metabolic pathways, lipolysis, and adipose-related signaling.
Research models show Tesamorelin may influence IGF-1 activity, enhance lipolytic gene expression, and support reductions in visceral adipose tissue (VAT). It is also being investigated for cognitive benefits and improved metabolic function in experimental settings.
SwissChems provides Tesamorelin in 2mg lyophilized vials, lab-tested for ≥98% purity, sealed in tamper-proof, temperature-controlled packaging to ensure peptide stability and molecular integrity.
Disclaimer: All information on Tesamorelin is for educational purposes only. Consult a healthcare professional before conducting research on these compounds.

Tesamorelin Overview
⭐ Top Benefits: Supports adipose modulation, IGF-1 pathway activity, & metabolic regulation
💉 Form: 2mg lyophilized research peptide (1 vial)
⏱ Max Time Used: 4–6 weeks (research use)
💲 Average Cost: $27.95 – $255.95
❤️ Side Effects: Mild injection-site irritation, transient appetite changes
⚠️ Dangers: May elevate IGF-1 signaling; limited long-term human safety data
🔗 Best Peptide Stack: Ipamorelin, CJC-1295 (no DAC), AOD-9604
♂♀ Men/Women: Suitable for both (research use)
Copy Brawn20 for 20% off
- Supports reduction of visceral adipose markers in research models
- Enhances metabolic pathway activation (GHRH → GH → IGF-1 axis)
- Synergizes well with fat-loss peptides in experimental use
- High purity & stable lyophilized format
- Requires precise reconstitution and handling
- IGF-1 modulation requires cautious use
- Very limited long-term safety data
- Higher cost compared to other metabolic peptides
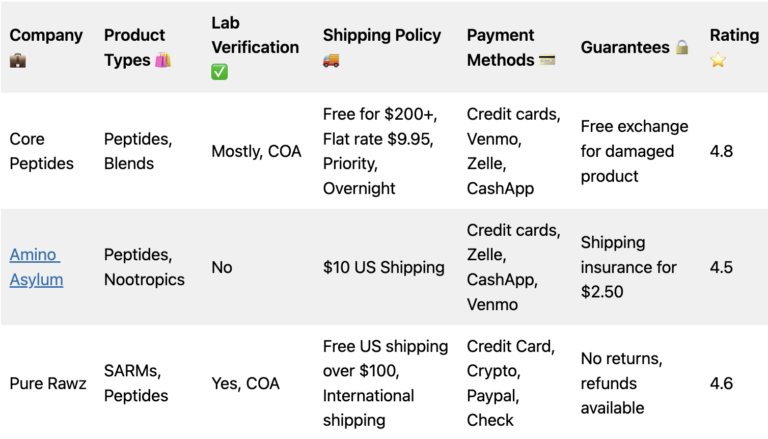
Where to Buy Tesamorelin
With Peptide Sciences shutting down, a lot of people are scrambling for reliable peptide sources. The landscape has shifted, but there are still solid options. I’ve broken down the best Peptide Sciences alternatives in a separate piece if you want the full picture.
For tesamorelin specifically, here are the vendors I’d actually recommend:
Swiss Chems is my go-to. They’ve been consistent with purity, their COAs are verifiable, and the 2mg vials are priced fairly for the quality you get. If you’re comparing Peptide Sciences vs Swiss Chems, Swiss Chems wins on availability alone now.
Behemoth Labz is another option I’ve had positive experiences with. Competitive pricing and they publish their testing results.
Sports Technology Labs rounds out the top three. Known more for SARMs, but their peptide line has been solid. Good option if you’re already ordering other compounds from them.
Tesamorelin FAQ’s
What is the recommended tesamorelin dosage per day?
The FDA-approved tesamorelin dosage is 2mg per day, administered as a single subcutaneous injection. Many users in the anti-aging and fitness communities start at 1mg daily and work up to the full 2mg dose. This should be taken on an empty stomach, either before bed or first thing in the morning.
How long does it take for tesamorelin to work?
Most users report noticeable changes in body composition around weeks 8-12. However, IGF-1 levels typically rise within the first 2-4 weeks, and improvements in sleep quality and recovery can be felt earlier. The clinical trials ran for 26 weeks, with the most significant fat reduction measured at that endpoint.
Can you take tesamorelin twice a day?
Splitting the dose isn’t standard protocol and isn’t supported by clinical data. The 2mg once-daily dosing was used in all major clinical trials. Some users have experimented with 1mg twice daily, but there’s no evidence this produces better results than a single daily injection, and it doubles the number of times you’re pinning.
Does tesamorelin need to be cycled?
While there’s no strict requirement to cycle tesamorelin, most users run it for 12-26 weeks followed by 4-8 weeks off. This approach helps maintain pituitary sensitivity to the compound. Some anti-aging clinics prescribe it continuously under medical supervision with periodic blood work monitoring.
What happens when you stop taking tesamorelin?
Unfortunately, the fat reduction benefits tend to partially reverse after discontinuation. In the clinical trials, visceral fat began to increase again once subjects stopped tesamorelin. This is why some people opt for periodic maintenance cycles rather than a single run. Your natural GH production returns to baseline fairly quickly — usually within 1-2 weeks.