Exemestane is one of the most widely used aromatase inhibitors in the bodybuilding community. It is prescribed clinically for hormone receptor-positive breast cancer in postmenopausal women, and in performance contexts it is used primarily to manage estrogen during anabolic steroid cycles and as part of post-cycle therapy.
How Does Exemestane Work?
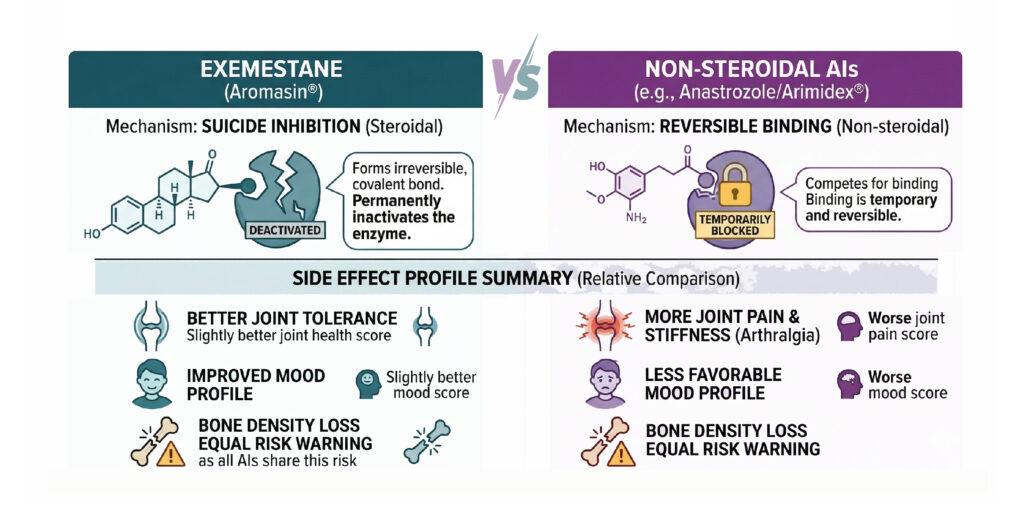
Exemestane is a steroidal aromatase inactivator. It works through suicide inhibition: it permanently and irreversibly binds to the aromatase enzyme, destroying it.
Suicide inhibition sounds dark, but it’s a reference to a biological process. Sometimes, an enzyme accidentally binds to the wrong molecule. This molecule looks close enough to the real thing that the enzyme starts processing it normally. But partway through, the two get permanently stuck together.
Once that happens, the enzyme can’t do its job anymore. It’s essentially been switched off by the very process it was designed to carry out.
Scientists call this “suicide inhibition” because the enzyme, in a sense, deactivates itself. It’s not damaged from the outside. It just gets caught in its own mechanism.
New estrogen production can only resume when the body synthesizes new aromatase enzyme from scratch. This means it is more aggressive in its estrogen suppression than reversible inhibitors.
That potency is part of what makes it effective, and part of what makes understanding its side effect profile genuinely important. Estrogen is not simply a female hormone to be eliminated. It plays critical roles in bone density, cardiovascular function, joint health, lipid metabolism, libido, and mood in both sexes. When you suppress it aggressively or for extended periods, you create real biological consequences.
This article goes through exemestane’s side effect profile systematically, drawing on clinical trial data rather than anecdote, and contextualizes the risks clearly for both the clinical and bodybuilding use cases.
Key Points
- Exemestane is a steroidal suicide inhibitor of aromatase, permanently inactivating the enzyme rather than reversibly blocking it, which makes estrogen suppression more sustained and potent than with anastrozole or letrozole. 🔬
- Bone density loss is the most clinically documented serious side effect, occurring even with calcium and vitamin D supplementation. DEXA scans before and after extended use are strongly recommended. 🦴
- Joint pain, fatigue, hot flashes, and headache are the most commonly reported daily side effects, consistent across multiple clinical trials at the standard 25 mg dose. 📋
- Exemestane’s mild androgenic activity (due to its steroidal structure resembling androstenedione) gives it a somewhat more favorable joint and mood profile compared to non-steroidal AIs, but does not eliminate the risks of estrogen suppression. 💊
- Liver enzyme elevations and lipid changes have been documented in trial data. Periodic bloodwork covering a full lipid panel and liver function tests is essential for anyone using exemestane beyond short on-cycle management. ✅

What Is Exemestane and Why Do Bodybuilders Use It?
Exemestane is classified as a Type I steroidal aromatase inactivator. Structurally it is a modified androstane steroid, chemically known as 6-methylideneandrosta-1,4-diene-3,17-dione, which is similar to the natural aromatase substrate 4-androstenedione.
This structural resemblance is what enables it to act as a false substrate, binding to aromatase and triggering a reaction that permanently inactivates the enzyme.
In clinical medicine it is FDA-approved at 25 mg once daily for postmenopausal women with hormone receptor-positive early or advanced breast cancer. It is typically prescribed after two to three years of tamoxifen therapy as part of a sequential adjuvant hormonal treatment approach.
In bodybuilding contexts, exemestane is used for two main purposes. During anabolic steroid cycles, elevated testosterone and other androgens undergo aromatization to estrogen. Without estrogen management this can lead to water retention, gynecomastia, and high blood pressure.
Exemestane is used on-cycle to suppress this excess estrogen conversion. Post-cycle, it is sometimes used as part of PCT to manage estrogen rebound as exogenous androgens clear and the hypothalamic-pituitary axis recovers.
Its advantage over reversible aromatase inhibitors in the bodybuilding context is partly its steroidal structure, which gives it mild androgenic activity and a somewhat more favorable profile for joint health and mood compared to anastrozole or letrozole.
Its disadvantage is the same property that makes it effective: permanent enzyme inactivation means the estrogen suppression is harder to reverse quickly if you overshoot and crash your estrogen. Understanding the side effects that come with that mechanism is critical for using it responsibly.
Bone Density Loss
This is the most serious and best-documented long-term side effect of exemestane and aromatase inhibitors as a class. Estrogen plays a central role in bone metabolism in both sexes. It promotes osteoblast activity (bone building) and inhibits osteoclast activity (bone breakdown). When estrogen is suppressed, the balance shifts toward net bone resorption.
Clinical data shows exemestane causes statistically significant reductions in bone mineral density at multiple skeletal sites including the distal tibia, distal radius, lumbar spine, total hip, and femoral neck. Cortical thickness is reduced at both the distal tibia and distal radius.
Importantly, bone loss has been documented even in patients receiving calcium and vitamin D supplementation, indicating that standard supplementation alone cannot fully offset the effects of estrogen suppression on bone. Two years of treatment has been shown to meaningfully worsen the age-related bone loss that occurs in postmenopausal women.
The FDA label for exemestane explicitly warns that the drug decreases estrogen, which reduces bone mineral density over time and increases fracture risk. Bone monitoring is described as mandatory during treatment in clinical guidelines.
It is worth noting that in placebo-controlled prevention trials, no statistically significant increase in skeletal fractures was observed versus placebo (149 vs 143 events), which suggests the bone density changes do not always translate to immediate fracture risk increases at typical clinical doses.
However, this is a population of postmenopausal women at a specific dose and duration, not necessarily reflective of extended use at other doses in male users.
For anyone using exemestane for extended periods, a DEXA bone density scan before starting and after each significant period of use is the clinically appropriate monitoring approach. For shorter on-cycle use at moderate doses, the bone density risk is less acute but not zero, particularly for users who are already not optimizing calcium, vitamin D, and weight-bearing exercise.
Joint Pain and Musculoskeletal Symptoms
Arthralgia (joint pain) and myalgia (muscle pain) are among the most consistently reported side effects of aromatase inhibitors across all clinical trials. In a 2024 ASCO analysis of postmenopausal breast cancer patients, arthralgias were reported by 79% of patients on non-steroidal AIs, making it by far the most common symptom in that group. Body aches were reported by 25%.
Exemestane’s steroidal structure gives it a relative advantage here. Because it has mild androgenic activity, it tends to produce less severe joint-related symptoms than anastrozole or letrozole.
The 2024 ASCO data showed that 51% of patients who switched from non-steroidal AIs to exemestane experienced a significant decrease in symptom severity, with improvements that were statistically significant across all menopausal symptoms. This switch benefit is one reason exemestane is frequently prescribed when patients cannot tolerate anastrozole or letrozole.
In bodybuilding contexts, joint pain from exemestane use is typically attributed to estrogen levels dropping too low. Estrogen has a lubricating and anti-inflammatory role in joint tissue.
When it is suppressed excessively, the loss of this protective effect can produce aching, creaking joints, and reduced range of motion. This is particularly relevant during strength training where joint stress is already elevated.
The practical takeaway is that exemestane’s joint profile is better than the non-steroidal alternatives, but joint symptoms are still dose-dependent and can emerge when estrogen is pushed too low. Monitoring how joints feel during use is one of the most accessible indicators that estrogen suppression may be exceeding an optimal level.
Estrogen Crash: The Risk Specific to Bodybuilding Use
This side effect is not prominently featured in clinical oncology literature because patients on clinical doses for breast cancer are trying to suppress estrogen as much as possible. In bodybuilding, the goal is different: manage excess estrogen without eliminating it entirely. Getting this balance wrong is one of the most common mistakes with aromatase inhibitor use.
An estrogen crash, also called estrogen rebound suppression, occurs when aromatase is inhibited too aggressively and estrogen levels fall below physiologically healthy levels. Symptoms include severe joint pain, significant libido loss, erectile dysfunction, emotional blunting and depression, brain fog, fatigue, inability to achieve muscle pump, and in some cases serious mood disturbances. These symptoms can be indistinguishable from low testosterone, which complicates diagnosis.
What makes exemestane particularly relevant here is the irreversibility of its mechanism. With anastrozole or letrozole, if you realize you have suppressed estrogen too much, stopping the drug allows aromatase to resume function within days as the reversible inhibitor clears. With exemestane, new aromatase enzyme must be synthesized before estrogen production can meaningfully recover. Recovery therefore takes longer, and simply stopping the drug does not produce rapid relief.
This is why dose titration is particularly important with exemestane. Standard bodybuilding protocols use lower doses than the clinical 25 mg daily: many on-cycle protocols use 12.5 mg every other day or every three days rather than daily dosing, calibrated to the aromatization level of the steroid stack being used. Bloodwork tracking estradiol (E2) levels before, during, and after an exemestane protocol is the most reliable way to avoid an estrogen crash.
Healthy estrogen levels in adult males typically fall in the range of 20 to 40 pg/mL for estradiol. Symptoms of low estrogen commonly appear when E2 drops below 15 to 20 pg/mL. Regular bloodwork is the most practical prevention tool.
Cardiovascular and Lipid Effects
Estrogen has protective effects on the cardiovascular system, including favorable effects on lipid metabolism, endothelial function, and vascular tone. Suppressing it pharmacologically has the potential to affect cardiovascular risk markers.
Clinical trials comparing exemestane to tamoxifen found higher incidences of cardiovascular events including angina and heart attack in the exemestane group, with a reported rate of 1.6% for exemestane versus 0.6% for tamoxifen. However, this comparison is complicated by tamoxifen’s known cardioprotective properties, meaning some of the apparent excess with exemestane may reflect a tamoxifen benefit rather than an exemestane risk. When exemestane was compared directly to placebo in prevention trials, no statistically significant difference in cardiovascular events was observed (106 vs 111 events, p=0.78), and stroke rates were similarly equal. This is a more reassuring picture for cardiovascular risk at standard clinical doses.
Lipid profile changes are more consistently documented. Clinical data shows exemestane is associated with elevated liver function test values and changes to lipid markers. In comparative data against tamoxifen, exemestane showed higher incidences of hypercholesterolemia. The mechanism is consistent with estrogen suppression impairing the favorable estrogen effects on HDL cholesterol and LDL clearance.
For bodybuilders who are also using anabolic steroids, which themselves cause significant lipid panel disruption (HDL reduction, LDL elevation), adding an aromatase inhibitor that compounds this effect is a meaningful cardiovascular risk consideration. A full fasting lipid panel before and after any cycle that includes an aromatase inhibitor is strongly advisable.
Common Daily Side Effects
The following side effects are documented in clinical trial data as occurring in more than 5% of patients at standard doses. For bodybuilding users, the relevant ones are those that reflect estrogen suppression rather than those specific to cancer patient populations.
Fatigue
Fatigue is listed among the most common side effects of exemestane in clinical documentation and in comparative data against tamoxifen. Estrogen contributes to energy metabolism and mood regulation in both sexes. In bodybuilding contexts, fatigue from low estrogen can reduce training capacity and overall drive. When fatigue appears during exemestane use and is unexplained by training volume or sleep quality, estrogen levels should be checked.
Hot Flashes
Hot flashes are reported in approximately 27% of clinical patients on exemestane and are a direct consequence of estrogen suppression affecting hypothalamic thermoregulation. In male users, this symptom is less commonly reported but does occur, particularly when estrogen levels are driven very low. It typically resolves when either the dose is reduced or discontinued.
Headache and Dizziness
Headache is listed among the most common adverse effects in exemestane clinical data. Dizziness is also documented. Both can reflect vascular changes associated with altered estrogen levels and are typically mild to moderate in severity. Hypertension is listed in the clinical adverse effect profile, which in a bodybuilding context may compound the blood pressure elevations already associated with anabolic steroid use.
Insomnia
Insomnia is among the documented common side effects of exemestane at standard doses. Estrogen plays a role in sleep quality and REM architecture. Sleep disruption from low estrogen is well-established in postmenopausal women and can occur in male users at sufficiently suppressed estrogen levels as well.
Nausea and Gastrointestinal Effects
Nausea is frequently cited as a common side effect of exemestane and is one reason the clinical recommendation is to take it after a meal. Taking exemestane with food reduces gastrointestinal discomfort and also improves oral bioavailability, since absorption is enhanced by dietary fat.
Clinical documentation notes that exemestane may increase the risk of gastric ulcers, particularly in patients using NSAIDs simultaneously or with a prior history of gastric issues.
Hair Thinning (Alopecia)
Alopecia is listed among the common side effects in clinical exemestane documentation. This can reflect both the estrogen-suppressing effects of the drug and, in the case of exemestane specifically, its mild androgenic activity given its structural similarity to androstenedione. Users with existing genetic susceptibility to androgenic hair loss may find exemestane compounds this tendency more than non-steroidal AIs.
Liver Effects
Exemestane is extensively metabolized in the liver by CYP3A4 and aldoketoreductases. Elevated liver function tests (LFTs) are listed among its common side effects in clinical documentation, with higher incidences compared to tamoxifen noted in trial data.
The National Library of Medicine’s LiverTox database characterizes exemestane as associated with a low rate of serum enzyme elevations during therapy and rare instances of clinically apparent liver injury.
In the rare cases documented, presentations included cholestatic liver injury appearing within weeks of starting the drug. Cases of acute liver failure have been reported in women on exemestane therapy, though the causal relationship in some of those cases was not definitively established. The overall assessment is that clinically significant hepatotoxicity from exemestane alone is rare.
Importantly, even with severe liver impairment (Child-Pugh C), the AUC of exemestane triples but adverse effects are not considered increased, and no dosage adjustment is specified. This is counterintuitive and worth noting, though it does not mean exemestane is appropriate in patients with significant liver disease.
For bodybuilders using oral anabolic steroids alongside exemestane, the cumulative hepatic load is a relevant concern. Liver function monitoring via bloodwork during any cycle involving multiple hepatically-metabolized compounds is standard practice for a reason.
Rare and Serious Side Effects
Beyond the more common side effects documented above, exemestane has been associated with a small number of rarer but more serious adverse reactions in post-marketing and case report data.
Severe Skin Reactions
Severe rash including erythema multiforme and acute generalized exanthematous pustulosis (AGEP) has been reported with exemestane, typically with early onset in the first weeks of use.
A PubMed case review documented cutaneous vasculitis specifically triggered by exemestane, with the authors noting that some patients may progress to severe vasculitis manifestations if the drug is not stopped promptly. Skin reactions of this severity are rare but require immediate discontinuation and medical evaluation.
Mood Disturbances and Depression
Significant mood changes including depression and emotional blunting are reported in post-marketing data for exemestane. Estrogen modulates serotonin and dopamine systems in the brain, and its suppression can produce meaningful mood and cognitive effects.
In clinical oncology practice these effects are monitored and managed. In self-administered bodybuilding contexts they can be mistaken for overtraining, low testosterone, or psychological issues rather than recognized as an aromatase inhibitor side effect.
Cardiac Events
As discussed in the cardiovascular section, the 1.6% incidence of cardiac events including angina and myocardial infarction in clinical trials represents a signal worth acknowledging, even though placebo-controlled data was more reassuring.
Patients with pre-existing significant cardiac disorders were excluded from the key early breast cancer clinical trials, meaning the risk in that subpopulation is not well characterized. For bodybuilders with pre-existing cardiovascular risk factors, this is a relevant caution.
Drug Interactions
Exemestane is metabolized by CYP3A4, and compounds that induce or inhibit this enzyme can meaningfully alter its plasma levels and effectiveness.
The most significant interaction documented in controlled research is with strong CYP3A4 inducers. Rifampicin reduced exemestane AUC by 54% and peak concentration by 41% in a single-dose study, effectively halving its availability.
Other strong CYP3A4 inducers expected to produce similar effects include carbamazepine and St John’s Wort. For a bodybuilder taking St John’s Wort as a mood support supplement alongside exemestane, the aromatase inhibitor may be substantially less effective than expected.
Conversely, while the CYP3A4 inhibitor ketoconazole was shown in a clinical trial to have no significant effect on exemestane levels, the general principle of caution around strong CYP3A4 inhibitors such as certain antifungals, macrolide antibiotics, and grapefruit applies.
Estrogen supplementation predictably reduces exemestane’s effectiveness by providing the very hormone it is suppressing. In bodybuilding this is rarely an issue, but it is worth noting for anyone combining exemestane with hormone replacement therapy or other estrogenic compounds.
How to Manage Exemestane Side Effects Responsibly
Several practical steps meaningfully reduce the risk profile of exemestane use in bodybuilding contexts.
Bloodwork is the single most important tool. A baseline panel before starting should include a full lipid profile, liver function tests, bone-specific markers if extended use is planned, and estradiol (E2). The same panel mid-cycle and post-cycle allows you to see what the compound is actually doing rather than guessing from symptoms. The NCIC MAP.3 trial protocol required vitamin D level testing before treatment, which is a sensible precaution for anyone planning extended AI use.
Dosing conservatively and only as needed is more important with exemestane than with reversible AIs, precisely because the suicide inhibition mechanism makes overcorrection harder to undo. Starting at the lowest effective dose and titrating based on bloodwork rather than symptoms alone is the approach that reduces estrogen crash risk.
Calcium, vitamin D3, and K2 supplementation throughout any period of AI use is standard clinical practice for a reason. These do not fully prevent bone density loss but they reduce it. Vitamin D3 at 2,000 to 5,000 IU per day and K2 at 100 to 200 mcg per day alongside adequate dietary calcium represents the minimum appropriate support.
Taking exemestane with food rather than fasted reduces gastrointestinal side effects and improves absorption. Weight-bearing exercise supports bone density during periods of estrogen suppression. Avoiding NSAID overuse reduces the risk of gastric complications given the exemestane-NSAID interaction noted in clinical documentation.
Finally, recognizing the symptoms of low estrogen specifically rather than attributing everything to other causes is important. Severe joint pain, mood crashes, crushing fatigue, and libido loss during exemestane use are most commonly signs that estrogen has been suppressed below a healthy level. These are not signs to push through. They are signs to test, assess, and adjust.
Conclusion
Exemestane is a well-characterized compound with decades of clinical data behind it. That data is a significant asset for anyone trying to understand its real risk profile rather than relying on anecdote. The side effects are real, documented, and dose-dependent. They are also largely manageable with the right preparation.
The most important shift in thinking for anyone using exemestane in a bodybuilding context is understanding that estrogen management does not mean estrogen elimination.
Estrogen is physiologically necessary at appropriate levels for bone health, cardiovascular function, joint integrity, mood, libido, and cognitive function. The goal of aromatase inhibitor use during a steroid cycle is to prevent excess, not to suppress completely.
Bloodwork, conservative dosing, appropriate supplementation, and knowing what low estrogen looks and feels like are the practical tools that separate responsible use from the kind that produces lasting harm. Exemestane used intelligently and monitored properly is one of the more manageable aromatase inhibitors in its class. Used without those guardrails, its irreversible mechanism makes overcorrection genuinely difficult to walk back.
Frequently Asked Questions
Is exemestane safer than anastrozole or letrozole?
Its steroidal structure and mild androgenic activity give exemestane a somewhat better profile for joint pain and some menopausal symptoms compared to non-steroidal AIs. Clinical data from 2024 showed significant symptom improvement when patients switched from non-steroidal to steroidal AIs. However, its irreversible mechanism means that if you suppress estrogen too far, recovery takes longer than with reversible inhibitors. Whether it is safer overall depends on individual response and how well the dosing is managed.
How quickly does estrogen recover after stopping exemestane?
Unlike reversible AIs where estrogen can recover within days of stopping, exemestane’s permanent enzyme inactivation means recovery depends on how quickly the body synthesizes new aromatase enzyme. This typically takes one to two weeks for meaningful recovery and several weeks for full normalization, which is longer than the reversible alternatives. This is why oversuppression with exemestane is harder to correct quickly.
What are the signs that exemestane has suppressed estrogen too much?
The most common signs of excessive estrogen suppression include severe joint pain and aching, significant loss of libido, erectile dysfunction in male users, crushing fatigue, emotional blunting or depression, brain fog, inability to achieve muscle pump during training, insomnia, and hot flashes. These symptoms can overlap with low testosterone, which is why bloodwork checking both testosterone and estradiol is the correct diagnostic step rather than guessing.
Does exemestane affect testosterone levels?
Yes, indirectly. By suppressing estrogen, exemestane removes negative feedback on the hypothalamic-pituitary axis from estrogen, which can modestly increase LH and FSH, leading to a mild natural testosterone elevation. A study in young adult males found exemestane suppressed estradiol by approximately 35% and estrone by approximately 70%. This is one reason it is used in PCT protocols: it can help restore the testosterone axis by lifting estrogen-mediated suppression while the HPGA recovers.
Do I need to take supplements while using exemestane?
Calcium, vitamin D3, and vitamin K2 are the minimum recommended supplements for anyone using exemestane beyond short-term on-cycle management. Clinical guidelines require vitamin D testing before starting exemestane therapy and recommend supplementation throughout. These do not fully prevent bone density loss but they reduce it. For on-cycle use alongside anabolic steroids, liver support (NAC, TUDCA) is also advisable given the cumulative hepatic load of multiple metabolized compounds.