Oral anabolic steroids have been part of the bodybuilding conversation for decades. They are synthetic derivatives of testosterone, engineered to be active when swallowed rather than injected, and their appeal has always been tied to convenience. No needles, no reconstitution, no complicated protocols. But the real question most people are asking is a practical one: do they actually work for cutting and bulking, and are the tradeoffs worth it?
The answer is not straightforward. Oral anabolic-androgenic steroids (AAS) vary widely in their mechanisms, potency, and intended applications. Some are better suited to building mass, others to preserving lean tissue during a caloric deficit. Understanding those distinctions is key to evaluating their effectiveness in either context.
This article examines what research and clinical data suggest about oral AAS in bulking and cutting phases, how these compounds work at a physiological level, and what the limitations of this approach look like in practice.
Key Points
- Oral anabolic steroids are 17-alpha alkylated testosterone derivatives that remain active after ingestion by resisting first-pass liver metabolism. 💊
- Compounds like methandrostenolone and oxymetholone have been shown in research to produce significant mass and strength increases, making them more relevant to bulking applications, though water retention is a notable factor. 💪
- Oxandrolone and stanozolol are more frequently studied in lean tissue preservation contexts, offering anabolic support without estrogenic water retention, which aligns with cutting phase goals. 🔬
- All oral AAS carry hepatotoxic risk due to 17-AA modification, as well as documented effects on cholesterol levels and endogenous testosterone suppression. ⚠️
- Most available research is conducted in clinical or therapeutic settings; findings should not be directly extrapolated to unsupervised performance or physique use without recognizing significant knowledge gaps. 📚

What Are Oral Anabolic Steroids?
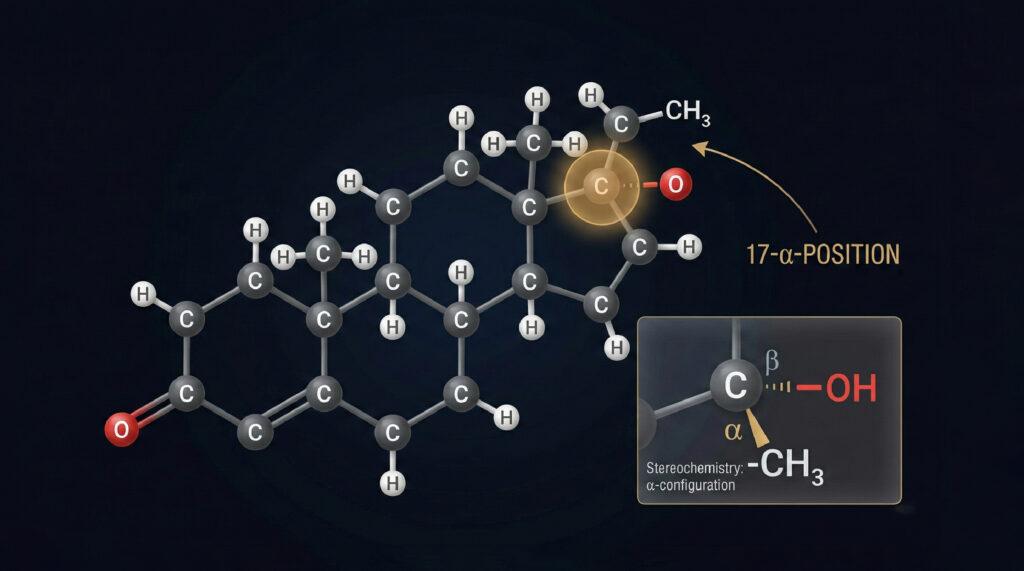
Oral anabolic steroids are synthetic compounds structurally derived from testosterone. Most of them are modified at the 17-alpha position of the steroid molecule, a chemical alteration that prevents rapid breakdown in the liver and allows the compound to remain active in the bloodstream after oral administration. This modification is commonly referred to as 17-alpha alkylation (17-AA).
The core function of anabolic steroids, regardless of delivery method, is to bind to androgen receptors in muscle tissue, stimulating nitrogen retention, protein synthesis, and cell proliferation. The anabolic-to-androgenic ratio varies between compounds, and that ratio largely determines whether a given steroid is better used during a mass-building phase or a leaning phase.
Common oral anabolic steroids studied in research and observed in athletic contexts include methandrostenolone (Dianabol), oxandrolone (Anavar), stanozolol (Winstrol), oxymetholone (Anadrol), and turinabol. Each has a distinct pharmacological profile.
Oral Anabolic Steroids for Bulking: What the Research Suggests
Bulking refers to a caloric surplus phase in which the goal is maximizing muscle hypertrophy and strength. Several oral AAS have been studied for their potential in this context, and the evidence points to meaningful but mechanism-dependent results.
Methandrostenolone (Dianabol)
Methandrostenolone is one of the most researched oral AAS in the context of muscle gain. Studies have shown it can significantly increase nitrogen retention and protein synthesis in skeletal muscle, which translates to rapid size and strength gains in a relatively short window. However, a substantial portion of the initial weight increase is attributed to intracellular water retention driven by estrogenic activity. This makes it effective for raw mass accumulation, though not ideal for those prioritizing lean, dry muscle gains.
Oxymetholone (Anadrol)
Oxymetholone is among the most potent oral anabolic steroids studied to date. Clinical research originally developed it for treating muscle-wasting conditions and anemia, and in those contexts, it demonstrated a strong capacity to increase muscle mass and red blood cell production. In research models, oxymetholone has been associated with some of the highest rates of mass accumulation among oral AAS, though it also carries a notable side effect profile and significant hepatotoxic potential due to its 17-AA structure.
Turinabol (4-Chlorodehydromethyltestosterone)
Turinabol was originally developed in East Germany and occupies an interesting middle ground. It does not aromatize to estrogen, which reduces water retention compared to methandrostenolone, and it has a lower androgenic ratio. Research data on turinabol is less abundant than some other compounds, but its profile suggests a slower, leaner mass gain pattern. Some researchers classify it as appropriate for either phase depending on dosage and context.
Oral Anabolic Steroids for Cutting: Preservation Over Growth
A cutting phase involves a caloric deficit intended to reduce body fat while preserving lean muscle tissue. The core challenge is that a hypocaloric environment is inherently catabolic, meaning the body tends to break down muscle for energy alongside fat. Anabolic steroids, in theory, counteract this by maintaining nitrogen balance and androgen receptor activity even under caloric stress.
Not all oral AAS are well-suited to this role. Those that cause significant water retention or estrogenic activity tend to mask the visual progress that defines a cutting phase. The compounds most frequently studied in lean tissue preservation contexts are those with a higher anabolic-to-androgenic ratio and minimal aromatization.
Oxandrolone (Anavar)
Oxandrolone is among the most studied oral AAS for lean tissue preservation and fat metabolism. It does not convert to estrogen, produces minimal water retention, and has a comparatively mild androgenic profile. Research in clinical populations including burn victims, elderly patients with muscle wasting, and HIV-positive individuals with weight loss has shown that oxandrolone can preserve lean body mass in catabolic states. These findings are frequently referenced in discussions about its potential relevance to cutting applications, though the research context differs significantly from a bodybuilding caloric deficit.
Stanozolol (Winstrol)
Stanozolol is a DHT-derived compound with a high anabolic-to-androgenic ratio and no estrogenic activity. It has been studied for its effects on strength and lean tissue retention without the fluid accumulation associated with more estrogenic steroids. In research settings, stanozolol has demonstrated effects on collagen synthesis and red blood cell production in addition to its anabolic actions. Because it does not cause estrogen-mediated water retention, it is often discussed in the context of phases where visible muscle definition is a goal.
Comparing Effectiveness: Bulking vs. Cutting Use Cases
The effectiveness of any oral AAS for bulking or cutting depends on several variables: the compound’s androgenic activity, its aromatization potential, the individual’s hormonal baseline, diet structure, and training volume. No compound works in isolation from these factors.
In general terms, oral AAS with higher estrogenic activity, such as methandrostenolone and oxymetholone, tend to show the most dramatic results in bulking contexts, particularly for raw weight and strength increases. However, those results often include significant water retention that can obscure muscle quality. Compounds like oxandrolone and stanozolol, which do not aromatize, are more frequently associated with cutting or recomposition goals, though their absolute hypertrophy effects are typically more modest.
It is also worth noting that oral anabolic steroids are generally considered less effective than injectable AAS for pure mass building, largely because their bioavailability and half-life are shorter and their hepatic strain limits the duration they can be used. This makes their relative effectiveness context-dependent in practical terms.
Safety Considerations and Research Limitations
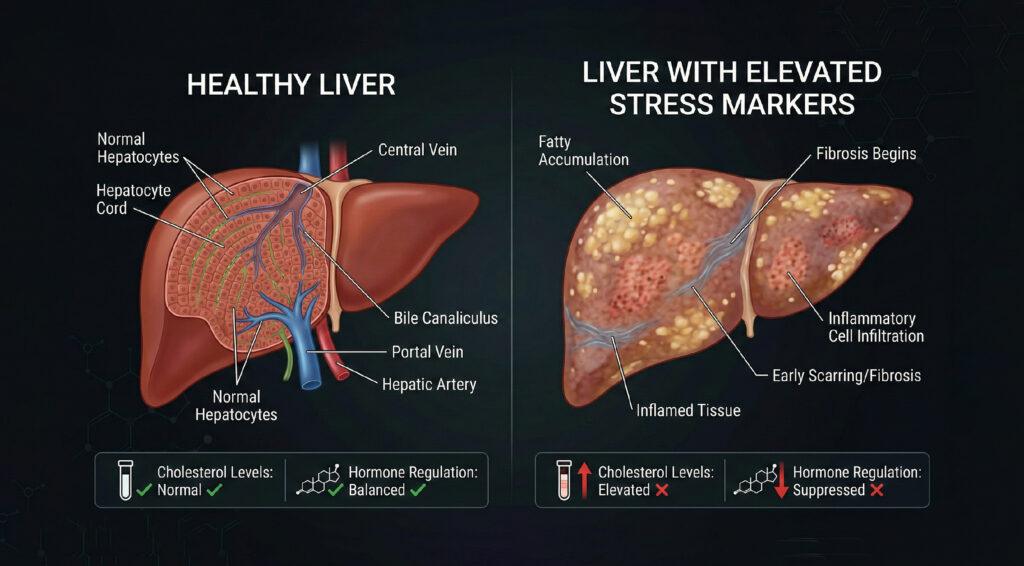
Any discussion of oral anabolic steroids would be incomplete without addressing the risks that accompany their use. The 17-alpha alkylation that makes oral AAS bioavailable also makes them more taxing on liver function. Studies have documented elevated liver enzymes, cholestasis, and in severe cases, hepatotoxicity associated with prolonged or high-dose oral AAS use. This is one of the primary reasons most clinical use of these compounds is time-limited.
Beyond hepatic effects, oral AAS have been studied for their impact on cardiovascular markers. Research has shown that they can reduce HDL cholesterol (the protective form) while elevating LDL, a pattern that is associated with increased cardiovascular risk over time. Endogenous testosterone suppression is another documented consequence, as exogenous androgens signal the hypothalamic-pituitary-gonadal axis to reduce natural hormone production.
It is also important to note that most available research on anabolic steroids has been conducted in clinical populations, often at therapeutic doses, and frequently under supervised conditions. Extrapolating these findings to performance or physique contexts introduces significant variables that the studies themselves did not account for. The long-term risk profile of supraphysiological oral AAS use in otherwise healthy individuals remains an area of incomplete research.
Oral anabolic steroids are controlled substances in many countries, including the United States, where they are classified as Schedule III controlled substances. This article does not advocate for their use outside of legitimate medical supervision and presents this information strictly for educational and informational purposes.
Conclusion
Oral anabolic steroids occupy a real and documented place in the research literature on muscle physiology. Their effectiveness for bulking or cutting is not a matter of speculation; it is a matter of which compound, at what dose, and in what physiological context. Mass-building steroids like methandrostenolone and oxymetholone have demonstrated the ability to accelerate hypertrophy and strength, while compounds like oxandrolone and stanozolol have shown value in preserving lean tissue under catabolic conditions.
What the research also makes clear is that effectiveness cannot be separated from risk. The 17-alpha alkylation that makes these compounds orally active is also responsible for their hepatotoxic potential. Cardiovascular effects and hormonal disruption are well-documented, even in supervised clinical settings. The gap between clinical research populations and real-world performance use is significant and should not be glossed over.
For those studying the science of anabolic compounds, understanding the pharmacological distinctions between these agents and their documented physiological effects is a valuable foundation. Whether that knowledge translates to legitimate research directions or informs a broader understanding of muscle biology, the nuance matters more than the headline.
Frequently Asked Questions
What is the difference between oral and injectable anabolic steroids?
Oral anabolic steroids are chemically modified to survive digestion and liver metabolism, while injectable versions typically bypass this process entirely. Because of the 17-alpha alkylation in oral forms, they tend to have shorter active windows and greater hepatic strain compared to most injectable counterparts. Injectable AAS are generally considered more efficient for sustained anabolic effects over longer cycles.
How do oral anabolic steroids work in the body?
They bind to androgen receptors in skeletal muscle and other tissues, which activates pathways involved in protein synthesis, nitrogen retention, and muscle cell proliferation. Depending on the compound, they may also influence red blood cell production, bone density, and appetite. The degree of androgenic versus anabolic activity varies by compound structure.
Are oral anabolic steroids safe?
All oral anabolic steroids carry documented risks, most notably liver toxicity, adverse changes in cholesterol profiles, and suppression of natural testosterone production. Clinical research conducted under supervision at therapeutic doses shows varying degrees of side effects depending on the compound, dose, and duration of use. Long-term safety data in healthy, non-clinical populations using supraphysiological doses is limited.
What are the side effects of oral anabolic steroids?
Commonly studied side effects include elevated liver enzymes, reduced HDL cholesterol, increased LDL cholesterol, suppressed endogenous testosterone, and androgenic effects such as acne and hair thinning in susceptible individuals. Estrogenic side effects such as water retention and gynecomastia are more common with compounds that aromatize. Some of these effects are reversible upon cessation; others may persist.
Can oral anabolic steroids be used with other compounds?
In research and clinical contexts, some oral AAS have been studied in combination with other compounds, including selective estrogen receptor modulators (SERMs) or aromatase inhibitors to manage estrogenic side effects. Combining multiple hepatotoxic compounds is generally associated with heightened liver strain. Any use in combination contexts carries compounded risks and falls outside the scope of most available clinical research.
Disclaimer: This content is for informational and educational purposes only. Oral anabolic steroids are controlled substances in many jurisdictions and are not approved for performance enhancement or physique modification by regulatory authorities including the FDA. This article does not constitute medical advice. Consult a licensed healthcare provider before making any decisions related to hormone-affecting compounds.