Are experiencing some symptoms like mood changes, erectile dysfunction, loss of libido, muscle loss, and fat gain?
You’ve heard about free testosterone, total testosterone, sex hormone binding globulin, and you are so overwhelmed you might as well give it all up – maybe this is how you’re supposed to feel.
Perhaps not… have no worries, we’ve got your back, and we’re gonna teach you all about SHGB, and how to lower SHGB.
Key Takeaways
- Almost 98% of the total testosterone is bound to plasma proteins.
- Bioavailable testosterone refers to both free testosterone and albumin-bound testosterone.
- Sex hormone binding globulin (SHBG) accounts for 60% of testosterone binding.
- Dietary composition changes, certain supplements and medications may contribute to lowering SHBG levels.
- Always remember that what works for other people doesn’t necessarily work for you. So, you need to consult with your doctor or healthcare provider first before changing anything in your diet and having any medication or supplement prescribed.
What Is Testosterone?
Testosterone is an essential, vital sex hormone for males, required for differentiation, and developmental growth. [2] Testosterone is crucial hormone for men due to its contribution to libido, mass muscle, fat distribution, mood, energy and sexual function. [3]
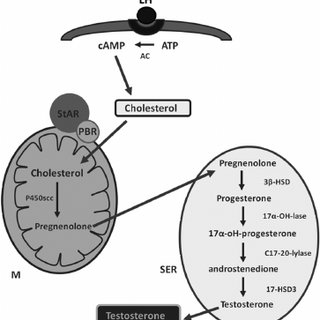
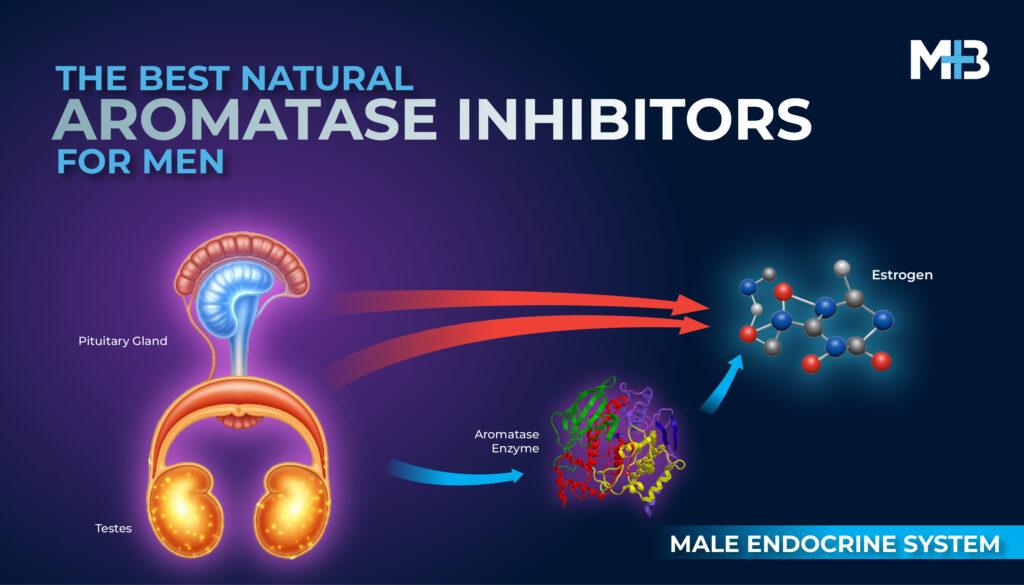
Testosterone is mainly (90%) produced by Leydig cells within the testes. Gonadotropin‑releasing hormone (GnRH), released by the hypothalamus regulates the pituitary production of luteinizing hormone (LH) and follicle‑stimulating hormone (FSH). [3]
LH stimulates the production of testosterone while FSH binds to Sertoli cells and promotes spermatogenesis. [3]
Approximately 10% of male androgens are produced by the adrenal glands. [3]
Testosterone is metabolized to dihydrotestosterone (DHT) and estradiol (E2) ‑ active metabolites that provide negative feedback at the level of the pituitary. [3]
Normal Testosterone Levels
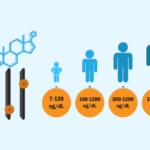
In young, healthy men (20 – 30 years old), the normal levels of serum testosterone (400 – 700 ng/dL) are controlled by the feedforward and feedback components of the hypothalamic-pituitary-gonadal axis and are maintained within the normal range of 300–800 ng/dL. [2]
Total Testosterone
Testosterone exists in the bloodstream in two forms, bound and free. [3]
Total testosterone refers to all forms of testosterone in the serum. [3]
Bound Testosterone
The vast majority of testosterone is bound to plasma proteins, representing 97-98% of total testosterone. [3]
About 33-54% of the total testosterone that is complexed to albumin is weakly bound and has androgenic potential. [3]
Approximately 44-65% of the total testosterone bound to sex hormone binding globulin (SHBG) is tightly bound and is essentially inactive. [3]
Free Testosterone
Represents only 2-3% of the total testosterone. [3]
When SHBG level goes up, free testosterone levels go down.
The free testosterone is thought to be the component that has access to cells and possesses androgenic action. [3]
By measuring total testosterone, SHBG and either assuming an albumin value or measuring it, a free testosterone calculation can be performed. [3]
Bioavailable Testosterone
Bioavailable testosterone refers to both free testosterone and albumin-bound testosterone. [3]
The levels of bioavailable testosterone are inversely related to the levels of SHBG. [1]
The administration of testosterone has been the major treatment for the decline in bioavailable testosterone. [1]
Another approach to increase the bioavailable testosterone would be to decrease the levels of SHBG, which is influenced by a wide range of factors, such as age, weight, and diet. [1]
Testosterone Deficiency
Testosterone Deficiency, also known as Androgen Deficiency in the Aging Male (ADAM), hypogonadism and andropause is estimated to affect 10% of men older than 30 years of age and up to 40% of men older than 70 years of age. [3]
The decline in total testosterone levels in men as they age, has been shown to affect a number of factors such as sexual function, bone density, and lipid profiles. [1]
The decline in total testosterone is accompanied by a decline in the free and bioavailable testosterone and the decline in the latter fractions is amplified by a concomitant increase in sex hormone-binding globulin levels. [1]
It is now well established that testosterone deficiency negatively impacts sex drive, erectile function, energy levels, mood, cognition, muscle mass, bone density and fat accumulation. [3]
Major Causes of Low Testosterone Levels
Primary testicular failure: a decrease in testicular function with age. [4]
Secondary testicular failure: a decrease in hypothalamic-pituitary axis function with a corresponding decrease in circulating gonadotropins. [4]
Increase in the production of sex hormone-binding globulin (SHBG). [4]
Signs and Symptoms of Low Testosterone Levels
- Anemia.
- Depressed mood.
- Erectile dysfunction.
- Decreased libido and sexual desire.
- Reduced muscle mass and strength.
- Reduced bone mass and osteoporosis.
- Insomnia and a reduced sense of general well-being.
- Forgetfulness, difficulty in concentration, and loss of memory.
What is Sex Hormone Binding Globulin?
Sex hormone-binding globulin, also known as testosterone-binding globulin or sex steroid binding globulin, is a glycoprotein produced by the liver and binds to sex hormones and carries them through the blood. [5]
It participates in the regulation of estrogen and testosterone by affecting free hormone availability and uptake by the target organs.
Sex hormone binding globulin (SHBG) accounts for 60% of testosterone binding, and 40% of the total testosterone is bound by albumin or other proteins. [6]
Total testosterone concentrations are influenced by alterations in SHBG concentrations. [7]
Most of the circulating testosterone is bound to SHBG and to albumin. [7]
What Hormones Bind to SHBG?
- Testosterone, the main sex hormone in men.
- Dihydrotestosterone (DHT), another male sex hormone.
- Estradiol, a form of estrogen, the main sex hormone in women.
SHBG Blood Test
Although SHBG attaches to all three of these hormones, an SHBG test is mostly used to look at testosterone. SHBG level can show if there is too much or too little testosterone being used by the body. [8]
Sometimes a total testosterone test is enough to make a diagnosis. But some people have symptoms of too much or too little of the hormone that the total testosterone test results can’t explain. In these cases, an SHBG test may be ordered to provide more information about how much testosterone is available to the body. [8]
Functions of SHBG
Maintaining and stabilizing the availability of unbound sex hormones. [5]
Sex hormones transport: SHBG-bound testosterone is not available for transport into tissues; SHBG-bound estradiol is available for transport into liver, salivary gland, and lymph node. [9]
What are the Conditions where SHBG Levels are Low?
Here are few examples of clinical disorders that cause elevated SHBG levels dropped [8]:
- Testicular cancer
- Type II diabetes mellitus
- Overuse of steroid medications
- Cushing’s syndrome: A condition in which your body makes too much cortisol
- Polycystic ovarian syndrome (PCOS): A hormone disorder affecting childbearing women
- Hypothyroidism: A condition in which your body doesn’t make enough thyroid hormones
What are the Conditions where SHBG Levels Are High?
Here are few examples of clinical disorders that cause elevated SHBG levels [8]:
- Liver disease
- Eating disorders
- Pituitary gland disorders
- Hyperthyroidism: A condition in which your body makes too much thyroid hormone
What Is the Normal Range of SHBG Levels?
The normal range of SHBG in the blood of adult men is 10-50 nmol/L. [10]
So, Why Do You Need to Lower Your SHBG Levels?
A SHBG level that is too high may cause symptoms of low testosterone even when the total testosterone levels are within normal range. It can also worsen symptoms when the total testosterone level is already low.
So if you have all the symptoms of Low testosterone like tiredness, low libido, erectile dysfunction, loss of muscle strength etc and yet your total testosterone level are within normal, it could be due to low free testosterone.
Now if your free testosterone is low because your SHBG is too high, you may not want to receive yet exogenous testosterone to solve the problem. You may instead want to try to lower your SHBG levels first.
How To Lower Your SHBG Levels?
Dietary Composition
Several small scale studies of the relation between dietary composition (fiber, caloric, and protein intake) and SHBG levels show conflicting results. [1]
The dietary components that correlated best with SHBG levels were protein and fiber. [1]
High Fiber Diet
In women, a high fiber diet was shown to decrease SHBG levels. [1]
High Caloric Intake
In another study, women with anorexia who were given increased calories had a decrease in SHBG levels, whereas other research indicates that a very low calorie diet results in a doubling of SHBG levels over a short term in women with polycystic ovary syndrome. [1]
High Fat Diet
Reed et al. noted that normal men fed a high fat diet had a decrease in SHBG levels, whereas a diet low in fat resulted in an increase in SHBG levels. [1]
Protein Intake
The higher the protein intake, the lower the concentration of SHBG. [1]
One of the major controlling factors on SHBG synthesis is insulin. This intake of protein has been shown to increase serum insulin levels, and insulin has been shown to reduce SHBG levels. [1]
The inverse relationship between protein and SHBG suggests that in elderly men a high protein diet could increase bioavailable testosterone and mitigate the effects of the age-related decrease in testosterone. [1]
Supplements
Boron
Six hours boron supplementation had no major effect on hormone concentrations except SHBG showed significantly lower concentrations following boron consumption. [11]
Supplementation of healthy males with 10 mg/d after one week resulted in a significant rise in plasma free testosterone concentration. [11]
It is known that the major circulating androgen in males is testosterone and about 98% of testosterone molecules are bound to proteins in the blood, principally to sex hormone-binding globulin (SHBG) and also to albumin and cortisol-binding globulin. [11]
Elevation of unbound free testosterone by boron supplementation supports the hypothesis that boron has an important biological role or change in steroid utilization. [11]
Vitamin D
Vitamin D supplementation might increase testosterone levels in men. [12]
A previous study showed that in overweight men with deficient vitamin D status, a significant increase in testosterone was observed after intake of 83 μ g vitamin D daily for 1 year. [12]
Zinc
Zinc influences the functioning of the male reproductive system and it is involved in steroidogenesis, promotes the maturation of sperm and, regulates the concentration of dihydrotestosterone formed from testosterone. [13]
Zinc deficiency may cause hypogonadism, decreased testosterone levels, impaired fertility and reduced sperm viability and quantity. [13]
Hormone Replacement Therapy
It’s been reported before that the administration of exogenous testosterone may cause the body to down regulate its SHBG levels. This has been found to work on men who have low testosterone levels.