You hit your protein goal, crushed your steps, and kept calories tight. Then late‑night hunger steamrolls your plan. That’s not a discipline problem. It is a weak signal between your gut and your brain. Fixing the signal and sticking to the plan gets easier.
Oleoylethanolamide (OEA) is a fat‑derived messenger your small intestine makes. A strong OEA signal helps you feel full sooner and stay satisfied longer between meals. It also guides how the body uses fat for energy. In simple terms, OEA supports appetite control while you follow solid habits.
Human studies show early, promising results. Several trials report lower hunger scores and small drops in body weight and waist size over weeks. Researchers link these effects to PPAR‑alpha activation. OEA also talks to the brain through the vagus nerve and the hypothalamus, which helps manage appetite.
OEA is not a magic pill. It works best when the basics are in place: high‑protein meals, fiber, daily steps, and strength training. This guide keeps the science clear and practical. You will learn how to test OEA safely and see if it helps you control appetite and keep a steady calorie deficit.
Key Takeaways
- OEA helps control appetite and supports fat use through PPAR‑alpha, which makes a calorie deficit easier to keep. 🔁
- Best results come with high protein, fiber, daily steps, and steady strength training. Basics first. 🧱
- Most human trials use 125–250 mg/day for 8–12 weeks; start low and track hunger, weight, and waist. 📊
- Signals include better insulin sensitivity and calmer oxidative stress markers, but results are modest and built with consistency. ⏳
- If hunger does not drop or side effects appear, stop and reassess with a clinician before continuing. 🧭

What Is OEA?
Oleoylethanolamide is a bioactive lipid amide that your gut makes from oleic acid in dietary fat. It acts locally in the small intestine and in the brain through the gut-brain axis. Researchers study oleoylethanolamide weight loss because OEA helps control food intake and body weight. Endogenous OEA interacts with adipose tissue and may influence body composition over time.

OEA’s core mechanism is PPAR-α activation. This supports fatty-acid oxidation and cleaner lipid metabolism. In simple terms, OEA nudges the body to use fatty acids for energy instead of storing them. Many papers describe the effect of OEA on energy metabolism and metabolic pathways linked to fat use.
OEA shows anti-inflammatory effects in models of diet-induced obesity. Studies report changes in inflammatory markers such as tumor necrosis factor-α (TNF-α) and other inflammatory factors. Researchers also track oxidative stress markers like reactive oxygen species (ROS) and lipid peroxidation. Some work notes higher antioxidant enzymes and reduced systemic inflammation after OEA treatment.
Others note a significant improvement in energy expenditure and intestinal motility, which also supports weight loss. These findings appear in diet-induced obesity models and align with lower chronic inflammation, calmer inflammatory factors, and stronger immune responses after OEA treatment.
Key pathways at a glance:
- OEA activates the proliferator activated receptor alpha and supports fatty acid oxidation.
- OEA stimulates lipolysis, guides lipid metabolism, and may increase energy expenditure.
- OEA supplementation reduces inflammation and oxidative stress in several models, including obese patients newly diagnosed with metabolic syndrome.
- OEA can lower inflammatory biomarkers and raise anti-inflammatory cytokines, which supports the innate immune response.
- OEA may influence gut microbiota and intestinal cytokines in high fat diet settings, which can shape hunger and food choices.
OEA works best when you combine it with sound dietary interventions and training. The effect of OEA builds when protein intake, steps, and sleep are consistent. As research grows, we will learn where OEA supplementation fits across different populations and inclusion criteria, from overweight adults to inflammatory disease contexts.
How Oleoylethanolamide Weight Loss Works Through the Gut-Brain Axis

Here is the simple view of how oleoylethanolamide supports weight loss. OEA adjusts hunger signals in the gut and brain, shifts how the body uses fatty acids, and calms low grade inflammation. These changes make it easier to eat less and keep a steady calorie deficit.
Appetite and Satiety via the Gut-Brain Axis and Gut Microbiota
OEA forms in the small intestine after you eat dietary fat, especially oleic acid. It signals fullness, so you stop sooner and wait longer before the next meal. This signal travels along the vagus nerve to the hypothalamus. Some users report fewer cravings and a calmer appetite within days. Research also notes shifts in intestinal motility, gut microbiota, and intestinal cytokines, which influence food intake and the innate immune response.
PPAR-α, Fatty Acids, and the Effect of OEA on Fat Use
OEA activates peroxisome proliferator-activated receptor-α (PPAR-α). This switch supports fatty acid oxidation and cleaner lipid metabolism. In simple terms, the body burns more fatty acids for energy and stores less. OEA may also stimulate lipolysis in adipose tissue and can support a small rise in energy expenditure over time.
This pathway helps explain oleoylethanolamide weight loss signals seen in studies and why oleoylethanolamide stimulates lipolysis during OEA treatment. This peroxisome proliferator-activated receptor-α (PPAR-α) pathway favors oxidation of unsaturated fatty acids, and benefits grow with consistent OEA treatment.
Inflammation and Oxidative Stress, Inflammatory Markers, and Immune Responses
Chronic inflammation and oxidative stress can blunt fat loss and raise disease risk. OEA shows anti-inflammatory effects in several trials and models. Researchers report lower inflammatory markers like tumor necrosis factor-α (TNF-α) and better oxidative stress markers.
Some studies also note improved insulin sensitivity and small but meaningful changes in body weight, waist size, and other metabolic parameters. Findings include lower lipid peroxidation and ROS, with higher antioxidant enzymes. These changes reduce systemic inflammation, improve insulin resistance, and support metabolic syndrome management.
What OEA Does Not Do for Body Weight and Body Composition
OEA is not a stimulant or a stand‑alone fat burner. It will not fix a high‑calorie diet or poor sleep. Think of it as an appetite and metabolism helper. The best results still come from protein‑forward meals, steps, and strength training.
Quick Cause and Effect
| What changes with OEA | Primary effect | Why this matters for weight loss |
| Stronger OEA gut and brain signal | Earlier fullness and less food intake | Fewer calories with less hunger and fewer cravings |
| PPAR-α activation | More fatty acid oxidation and smoother lipid metabolism | The body uses fatty acids for energy instead of storing them |
| Lower inflammation and oxidative stress | Improved insulin sensitivity and energy metabolism | Easier weight loss and better metabolic parameters |
| Consistent habits and OEA | Significant reduction in appetite and gradual change in body weight and body composition | A steady calorie deficit feels easier to keep |
Across RCTs, intervention groups often show decreased hunger, weight, BMI, and waist, with higher PPAR-α expression.
What the Research Says
Human data is small but growing. Most trials use 125–250 mg/day OEA for 8–12 weeks. Results often show a significant decrease in appetite and small but measurable changes in body weight, waist size, and fat mass, especially with a calorie‑restricted diet. Effects on inflammatory biomarkers are mixed, but oxidative stress markers often improve.
In several cohorts of obese patients, OEA supplementation produced significantly reduced tumor necrosis factor α and improved insulin sensitivity alongside better metabolic parameters. Researchers report these outcomes under clear inclusion criteria with standard statistical analysis, and benefits are usually strongest in the intervention group.
Key Trials in High Fat Diet and Diet-Induced Obesity Models
| Study & population | Dose & duration | Main outcomes |
| Obese adults (RCT) | 250 mg/day, 8 weeks | Significant reduction in hunger, body weight, BMI, waist; significant increase in PPAR‑alpha expression. |
| Obese adults with newly diagnosed NAFLD (triple‑blind RCT) | 250 mg/day + calorie deficit, 12 weeks | Anthropometric and metabolic markers improved. Liver fat trends favored OEA but were not significant between groups. |
| Obese NAFLD patients on a low‑calorie diet (RCT) | 250 mg/day, 12 weeks | Significant increase in antioxidant enzymes; significant decrease in lipid peroxidation markers; no between‑group change in TNF‑α, IL‑6, hs‑CRP. |
| Healthy obese adults (RCT) | 250 mg/day, 8–12 weeks | Signals of improved lipid profile and fasting blood sugar; dietary intake patterns also shifted. |
| Meta‑analyses (2025) | Pooled RCTs | Significant reduction in weight, waist, fat mass, and oxidative stress; mixed but promising signals on inflammatory factors like TNF‑α and IL‑6. |
Several reports indicate oleoylethanolamide supplementation reduces inflammation and oxidative stress in adults with metabolic issues. Benefits tend to be stronger when diets are controlled and adherence is high.
Across studies, OEA supplementation was associated with significantly reduced tumor necrosis factor-α (TNF-α), lower oxidative stress markers, and higher anti-inflammatory cytokines in some cohorts, with the largest effects seen in obese patients and those newly diagnosed with metabolic issues.
How This Connects to Mechanism
OEA activates the peroxisome proliferator-activated receptor-α (PPAR-α). This supports fatty acid oxidation, lipid metabolism, and may stimulate lipolysis in adipose tissue. Better energy metabolism can improve insulin sensitivity. Trials also note changes tied to inflammation and oxidative stress, which matter for metabolic syndrome and cardiovascular disease risk.
What to Expect in Body Weight, Insulin Resistance, and Body Composition
You may notice earlier fullness and fewer cravings. Weight loss is modest and grows when you pair OEA with protein‑forward meals and daily steps. Watch blood sugar, waist size, and energy. If you see no meaningful change after 8–12 weeks, consider a stop or a different approach.
These brief notes sit outside the weight‑loss protocol but appear across OEA literature (preclinical and early clinical). They help explain the broader effect of OEA on energy metabolism and immune pathways.
- High fat diet and diet-induced obesity: OEA treated mice and mice fed obesogenic diets show improved lipid metabolism, reducing oxidative stress with higher antioxidant enzymes and lower lipid peroxidation.
- Inflammation and immune cells: studies track immune responses and inflammatory markers, including tumor necrosis factor α; some show anti inflammatory effects and significantly reduced cytokines after OEA supplementation.
- Acute contexts: reports explore acute liver injury and acute ischemic stroke models; findings center on immune cells, oxidative stress markers, and energy metabolism signals.
- Women’s health: small studies note decreased dysmenorrhea pain; more work is needed.
These signals support the rationale for oleoylethanolamide weight loss research and fit with the PPAR pathway.
OEA Dosage, Timing, and How to Take It
Most human trials use 125 to 250 mg of OEA per day. Start low and watch how your hunger changes for one to two weeks. Increase only if appetite control is still weak and side effects are absent. Stay within the range unless your clinician advises otherwise.
Timing
Take OEA 30 to 45 minutes before a meal. Many readers choose the largest meal of the day. Split doses before lunch and dinner if late-day cravings persist. Be consistent for at least four weeks.
With or without food
Take OEA with water 30–45 minutes before meals. Some people prefer a small amount of dietary fat with the meal for comfort. Because endogenous OEA derives from oleic acid and other unsaturated fatty acids, pairing with healthy fats in dietary interventions can feel natural. Track hunger, cravings, and fullness to see which method works better for you.
Forms and labels
Choose a product that lists the exact milligrams of OEA per capsule. Look for third‑party testing and clean excipients. Avoid blends that hide the true dose.
Simple 4-Week Ramp to Improve Body Weight and Body Composition
Stop if you feel nausea, reflux, or unusual discomfort. Talk to your clinician if you take lipid‑lowering drugs or have liver, gallbladder, or GI issues. Do not use during pregnancy or breastfeeding without medical advice. People with inflammatory disease or cardiovascular disease should speak with a clinician before use.
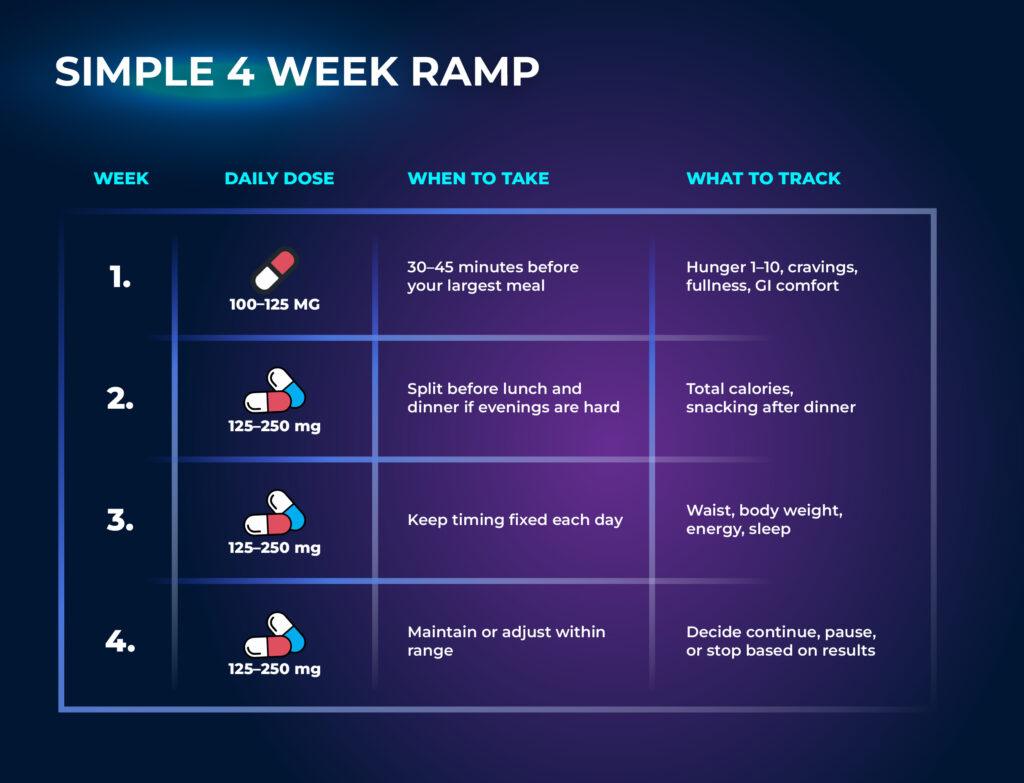
4 Week Practical Protocol
Use this four week plan to test if OEA helps you control appetite and improve your cut. Stay inside studied doses. Pair it with protein forward meals, steps, and strength work.
Week 1
Start at 100 to 125 mg per day. Take it 30 to 45 minutes before your largest meal. Log hunger before and after meals on a 1 to 10 scale. Hit a protein target and keep steps high. Note GI comfort.
Week 2
If appetite control is still weak, move toward 125 to 250 mg per day. You can split the dose before lunch and dinner. Keep calories steady and add fiber and water. Watch body weight, cravings, and sleep.
Week 3
Hold the dose within range. Train 2 to 4 days per week and keep steps consistent. Record waist, body fat trend, and energy. If you track labs, note fasting glucose or talk to your clinician about insulin sensitivity.
Week 4
Review the data. Look for a significant decrease in hunger and snacking. Expect a small change in body weight and waist if diet is on point. Decide to continue, pause, or stop.
Decision Guide
Continue if hunger drops by 2 or more points, snacks fall, and weight trends down 0.3 to 0.7 percent per week. Stop if you see no change or if side effects appear. Speak with a clinician if you have metabolic syndrome or complex meds.
What to Track
- Hunger ratings, meal size, food intake
- Body weight, waist, and a simple body composition estimate
- Energy, sleep, and training volume
- Side effects, GI comfort, and adherence
- In clinical settings, teams may track inflammatory markers like tumor necrosis factor-α (TNF-α), oxidative stress markers, and antioxidant enzymes
Stacking OEA for Better Results
A smart stack makes OEA work harder. You support appetite control and also push better energy metabolism. The goal is simple: fewer calories in, better fat use, and calmer inflammation.
Diet Synergy for Fatty Acids in High Fat Diet Contexts
Build meals around protein, fiber, and healthy fats. Oleic acid and other unsaturated fatty acids fit well with OEA’s pathway. This combo supports fatty acid oxidation and smoother lipid metabolism. Many readers also see steadier blood sugar and better insulin sensitivity.
Tips:
- Anchor each meal with 25–40 g protein.
- Add high‑fiber vegetables and fruit.
- Use olive oil or avocado for healthy fats.
- Drink water before meals to lower food intake.
Why it helps: Protein and fiber raise fullness signals. Healthy fats work with endogenous OEA and may steady gut microbiota and intestinal cytokines. Together they support anti-inflammatory effects and reduce chronic inflammation over time.
Training Synergy for Body Composition and Body Weight
Lift 2–4 days per week and keep steps high. Resistance training preserves muscle while you lose body fat and fat mass. Daily steps raise energy expenditure without heavy fatigue. These habits make OEA’s effect on fatty acids and lipid metabolism more visible.
Results to watch: Smaller waist and stable strength. A gradual but significant decrease in body weight when diet is controlled. Better insulin resistance markers and metabolic parameters when you stay consistent.
Light Stimulant Pairings (Optional)
You can pair OEA with coffee or green tea. Start small and avoid late‑day use. The aim is gentle appetite control and a slight lift in energy expenditure.
Caution: Skip heavy stimulant stacks. Monitor sleep, heart rate, and stress. Poor sleep raises inflammatory factors and blunts weight loss.
With GLP‑1 or Medical Protocols
Some obese patients on medical plans ask about OEA. Discuss this with a clinician. In supervised settings, diet plus OEA may help hunger control and insulin sensitivity. Teams should review inclusion criteria and use statistical analysis to judge real change.
Anti‑Inflammatory Support
Pair OEA with habits that lower systemic inflammation. Sleep 7–9 hours, manage stress, and include colorful plants. These steps can lower tumor necrosis factor α, reactive oxygen species (ROS), and lipid peroxidation while raising antioxidant enzymes. OEA supplementation may support reducing oxidative stress in parallel.

Keep it simple and measurable. OEA treatment works best with protein‑forward meals, regular lifting, and sleep. Over time you should see a significant reduction in hunger and gradual changes in body weight and waist as energy metabolism improves.
Who Might Benefit Most (and Who Should Skip)
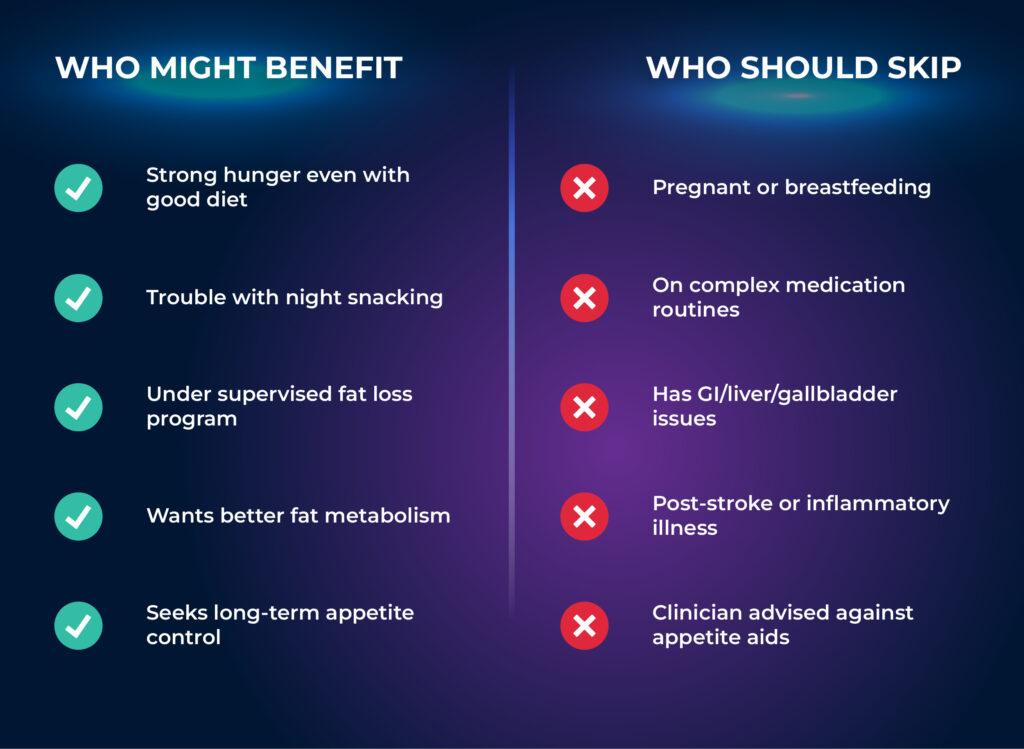
You are likely to benefit if you struggle with hunger on a calorie deficit. Portions creep up and late night cravings make you overshoot food intake. OEA may help you feel full sooner and wait longer between meals. Many obese patients under care also want support for insulin resistance and systemic inflammation. Clinicians often track insulin sensitivity, body weight, body mass index, waist size, and other metabolic parameters.
Signs you are a good fit
- Strong appetite on a cut despite solid protein and fiber
- High calorie environments at work or home
- Late night snacking that breaks the plan
- Elevated body weight or body mass index under a supervised program
- Interest in tools that support fatty acid oxidation, lipid metabolism, and energy metabolism
Use With Care
Talk to your clinician if you take drugs for blood lipids, blood sugar, or appetite. Discuss OEA if you live with metabolic syndrome, cardiovascular disease, or active inflammatory disease. Medical teams may choose to monitor inflammatory factors and other biomarkers during OEA supplementation.
Who should skip for now
- Pregnancy or breastfeeding
- Active GI, liver, or gallbladder disease, or a history of acute liver injury
- Recent acute ischemic stroke or complex medication routines
- Allergies or sensitivities to supplement ingredients
- Anyone advised by a clinician to avoid appetite agents
Why Some Should Avoid It
OEA acts through the PPAR pathway. This pathway influences fatty acids, lipid metabolism, and immune responses. Sensitive groups need medical oversight to avoid unwanted effects. When in doubt, do not start until your clinician clears it.
How to Measure Fit
Track hunger, cravings, and meal size each week. Watch body weight and waist. If you are under care, your clinician may track insulin sensitivity, inflammatory markers, and oxidative stress markers as well. Stop if you see no meaningful change after eight to twelve weeks of consistent use and sound habits.
Safety, Side Effects, and Interactions
Bodies respond differently. Start low and track your own response. Do not replace medical care with supplements.
Common Side Effects
Some users feel nausea, reflux, or stomach discomfort. A few report headache or light sleep when they pair OEA with caffeine. Lower the dose or move timing earlier if this happens. If symptoms persist, stop and speak with a clinician.
Why Mechanism Matters for Safety
OEA acts through the peroxisome proliferator activated receptor pathway. This pathway shapes lipid metabolism, fatty acids use, and energy metabolism. It also touches inflammation and oxidative stress. These effects help explain benefits and also why sensitive groups need guidance.
Possible Drug and Protocol Interactions
- Lipid‑altering drugs: pathways overlap with fatty acid oxidation and lipid metabolism. Coordinate with your clinician.
- GLP‑1 or appetite agents: combined use can push appetite too low. Monitor food intake and energy.
- Stimulants: caffeine or strong pre‑workouts may raise reflux or sleep issues. Keep doses modest and earlier in the day.
What to Monitor
Track hunger ratings, meal size, body weight, and waist each week. In clinical settings, teams may also track insulin sensitivity, insulin resistance markers, lipid profile, and inflammatory markers such as tumor necrosis factor α. Some studies also look at oxidative stress markers and antioxidant enzymes to confirm reducing oxidative stress.
Practical Safety Tips
Take OEA 30 to 45 minutes before a main meal. Begin at 100 to 125 mg. Increase only if appetite control is still weak and side effects are absent. Aim for four to eight weeks of consistent use before you judge results.
Red Flags
Stop and seek medical advice if you feel severe or persistent GI pain, vomiting, rapid unintended weight loss, or signs of very low energy intake. Do not rely on anti-inflammatory effects from OEA supplementation to replace medical care. Oleoylethanolamide supplementation reduces inflammation in some studies, but care plans for obese patients should still monitor metabolic parameters and overall health.
Comparing OEA to Other Weight Loss Aids
Oleoylethanolamide weight loss sits in the non-stimulant space. It works through the peroxisome proliferator-activated receptor-α (PPAR-α). The pathway supports fatty acid oxidation and cleaner lipid metabolism. Appetite control is the main effect of OEA.
If you want less hunger without jitters, OEA is a fit. Stimulants can cut appetite fast, but they may disrupt sleep and raise stress. Prescription tools can be powerful, yet they need medical oversight. Fiber is simple and safe, but slower. Below is a simple comparison table between OEA to other weight loss aids:
| Option | How it works | Pros | Watch outs |
| OEA (non-stimulant) | Signals fullness and activates peroxisome proliferator-activated receptor-α (PPAR-α) to support fatty acid oxidation and lipid metabolism | Lower food intake, calmer appetite, may aid insulin sensitivity and energy metabolism | Start low, track GI comfort, pair with diet and training |
| Caffeine and similar stimulants | Boosts alertness and can blunt appetite short term | Fast effect, easy access | Sleep issues, higher stress, tolerance, not ideal for chronic inflammation |
| Fiber supplements (psyllium, glucomannan) | Slows gastric emptying and increases fullness | Safe, helps lipids and blood sugar | Bloating if you add too fast, needs water and habit consistency |
| Green tea extract | Mild appetite and metabolic support | Gentle, common | Sensitive users may feel nausea or sleep disruption |
| Orlistat | Blocks fat absorption in the gut | Weight loss with diet support | GI side effects, fat soluble vitamin loss, medical advice needed |
| GLP-1 medications | Slows gastric emptying and reduces hunger signals | Strong appetite control, significant weight loss in trials | Requires prescription and follow up, possible GI side effects |
Where OEA Stands Out
You get appetite control without stimulant load. The effect of OEA fits cleanly with protein forward meals and steps. It may also support insulin resistance through better energy metabolism and lower inflammatory factors over time.
When Other Tools Make Sense
If hunger is extreme or metabolic disease is present, a clinician may prefer prescription options first. OEA can still support habits in a supervised plan. Fiber works for nearly everyone and can stack with OEA. Keep sleep and stress in check, as poor recovery drives systemic inflammation and overeating.
Final Thoughts
Oleoylethanolamide weight loss is not hype. It is a clear, testable approach that targets appetite and energy metabolism without stimulants. The effect of OEA runs through peroxisome proliferator-activated receptor-α (PPAR-α). This pathway supports fatty acid oxidation and cleaner lipid metabolism while you keep protein high, steps steady, and training on schedule.
Expect appetite relief first. Weight and waist decline when calories are controlled. Many readers also see better insulin sensitivity and calmer systemic inflammation over time, with shifts in oxidative stress markers. These changes are modest but meaningful when you stack them with good habits.
Hold a simple standard. If hunger drops, snacking falls, and weight trends down, keep going. If you see no change after eight to twelve weeks, or if side effects show up, stop and reassess. A clinician can help you review metabolic parameters and decide if OEA treatment fits your plan.
Bottom line: OEA helps you make the deficit stick. Use the four week protocol, measure what matters, and stay patient. Consistency beats intensity. Pair OEA supplementation with food quality, sleep, and training to turn small wins into real results.
Frequently Asked Questions (FAQs)
How does OEA affect sleep architecture over time?
OEA is non-stimulant; no evidence it changes sleep stages. Take it earlier in the day, avoid late caffeine, and reduce or stop if sleep worsens.
Is OEA appropriate for adolescents or older adults under medical supervision?
Adolescents: limited data. use only with a clinician. Older adults: start low, review meds, and monitor GI/liver/gallbladder history.
Does OEA change thyroid function or interact with iodine status?
No clinical evidence of thyroid effects; OEA acts via PPAR-α and lipid pathways. Not a thyroid aid. Ask your endocrinologist if you have thyroid disease.
Can OEA use influence fertility or menstrual cycle regularity?
No direct trials. Indirect effects can occur via weight, stress, or intake. Avoid in pregnancy/breastfeeding unless your clinician approves.
Does OEA interact with SSRIs, SNRIs, or other mood related medications?
Data is limited; check with your prescriber first. Monitor mood and sleep, and avoid stacking with strong stimulants.