Testosterone is still the king of anabolic steroids in 2026. Not the flashiest compound in the room, not the driest, not the strongest milligram for milligram, but it remains the foundation of almost every serious bodybuilding cycle.
There’s a reason most first cycles start with testosterone. It works consistently, it’s predictable compared to harsher compounds, and when diet and training are locked in, even moderate doses can produce dramatic changes in muscle mass, strength, recovery, and performance.
At the same time, modern discussions around testosterone use have shifted. In 2026, users are paying closer attention to cardiovascular health, estrogen management, fertility preservation, blood pressure, hematocrit, and long-term hormone recovery, not just scale weight and gym pumps.
This guide breaks down the best testosterone cycles for beginners and experienced users, explains the differences between esters like Enanthate, Cypionate, Propionate, and Sustanon, and covers modern cycle support, PCT strategies, and side effect management.
Key Points
- Testosterone remains the foundation of most anabolic steroid cycles in 2026. 💪
- Enanthate and Cypionate are still the most practical esters for mass gaining phases. 🏋️
- Propionate remains popular for cutting and contest prep due to faster clearance. 🔥
- Bloodwork and cardiovascular monitoring are now considered essential during cycles. ❤️
- Proper PCT and hormone recovery strategies matter just as much as the cycle itself. 🧪

What Are the Best Testosterone Cycles in 2026?
The best testosterone cycles depend entirely on the goal.
For leaner physiques and contest prep, many users still prefer Testosterone Propionate because of its shorter half-life and easier water management.
For off-season muscle growth, Testosterone Enanthate and Testosterone Cypionate remain the most practical choices due to stable blood levels and less frequent injections.
For TRT, cruising, or long-term hormone replacement, Cypionate and Sustanon continue to dominate because of convenience and predictable pharmacokinetics.
Quick Breakdown of the Most Popular Testosterone Esters
| Testosterone Ester | Best Use | Half-Life | Injection Frequency |
|---|---|---|---|
| Testosterone Propionate | Cutting, contest prep | ~4.5 days | Every other day |
| Testosterone Enanthate | Lean bulk, offseason | 7–9 days | 2x weekly |
| Testosterone Cypionate | TRT, bulking | ~8 days | 2x weekly |
| Sustanon 250 | Long-term cycles, TRT | ~15 days | 2x weekly |
What Testosterone Actually Is
Testosterone is the primary male androgen, which means it’s the hormone most responsible for everything we associate with being male, from muscle mass and bone density to libido, mood, drive, and red blood cell production. About 95% of it is produced in the testes by specialized cells called Leydig cells. The remaining 5% comes from the adrenal glands.
Its chemical signature is C19H28O2, a steroid hormone built from cholesterol. If your cholesterol is rock-bottom because you’ve been on an aggressive low-fat diet for years, your raw material for testosterone production is limited. The body literally cannot make hormones it doesn’t have the building blocks for.
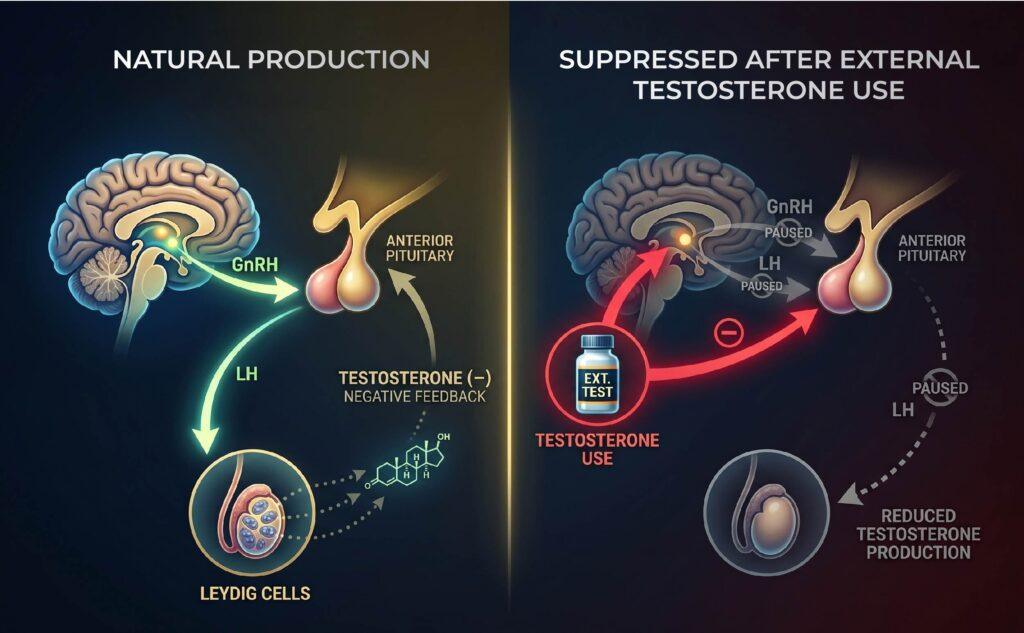
The whole testosterone production process is controlled by a feedback loop called the hypothalamic-pituitary-gonadal axis (HPTA or HPG).
Here’s how it works:
- The hypothalamus in your brain releases gonadotropin-releasing hormone (GnRH) in pulses throughout the day.
- GnRH tells the pituitary gland to release two hormones: luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
- LH travels to the testes and signals the Leydig cells to produce testosterone.
- FSH signals the Sertoli cells in the testes to produce sperm.
- As testosterone levels rise, the brain senses the change and dials down GnRH production — a classic negative feedback loop.
This loop is why anything that disrupts brain signaling like chronic stress, poor sleep, severe under-eating, and excessive alcohol, will eventually hits testosterone production. The testes are downstream of the brain. If the brain isn’t sending the signal, the factory isn’t getting orders to fill.
It’s also why introducing exogenous testosterone (the kind that comes from injections or gels) shuts down your natural production. Your brain detects high T in the bloodstream and stops signaling. The factory goes idle.
What Testosterone Converts Into

Testosterone doesn’t just exist as testosterone in your body. It converts into two downstream hormones that do critical work of their own. Unfortunately, they both get blamed for things they don’t actually deserve.
Dihydrotestosterone (DHT)
About 5 to 10% of your testosterone converts into DHT through an enzyme called 5-alpha reductase. DHT is significantly more potent than testosterone itself — roughly three to five times more androgenic at the receptor level. It’s what drives a lot of the visible “male” traits and a few of the less welcome ones:
- Facial and body hair growth
- Deepening of the voice (during puberty)
- Male pattern hair loss (in genetically susceptible men)
- Sebum and oil production in the skin
- Prostate growth
DHT got demonized because of the hair loss connection, but it’s not a villain. It’s essential for normal sexual function, libido, and overall male development. The guys who block DHT aggressively (with drugs like finasteride) often save their hair but pay for it with lower libido, mood issues, or post-finasteride syndrome in worst-case scenarios.
If you’re losing hair and considering DHT blockers, that’s a real conversation to have with a doctor who knows hormones, not a decision to make based on a Reddit thread.
Estradiol (Estrogen)
Testosterone also converts into estradiol through an enzyme called aromatase, most active in fat tissue. This is where the old-school bodybuilding mythology has done a lot of damage.
For decades, the narrative was that estrogen is the enemy. Crush it. Suppress it. Block aromatase as hard as possible. That approach is wrong, and the evidence has been piling up against it for years now.
In men, healthy estrogen levels are required for:
- Libido and erectile function
- Mood regulation and emotional stability
- Joint health and lubrication
- Bone density
- Insulin sensitivity
- Cognitive function
- Even muscle growth signaling
The problems happen at the extremes. Too much estrogen (usually from being overweight, since fat tissue ramps up aromatization) can cause water retention, mood swings, gynecomastia, and reduced libido. Too little estrogen, often from over-aggressive aromatase inhibitor use, causes joint pain, depression, zero libido, and a list of other miseries.
The body wants estrogen in a sweet spot, not on the floor. Anyone telling you to crush your estrogen is operating on outdated information.
What Are the Side Effects of Testosterone?
It’s worth nothing that the side effects are highly dose dependent and vary according to genetics, lifestyle, and ancillary support use. Like all anabolic-androgenic steroids, exogenous testosterone suppresses natural hormone production.
Common side effects include testicular atrophy, acne, oily skin, elevated hematocrit levels, increased blood pressure, and unfavorable cholesterol changes, particularly reductions in HDL (“good”) cholesterol and elevations in LDL (“bad”) cholesterol. Testosterone also converts into dihydrotestosterone (DHT), which may accelerate hair thinning or male pattern baldness in genetically susceptible users.
Because testosterone aromatizes into estrogen, some users may also experience water retention, bloating, or gynecomastia if estrogen levels become excessively elevated during a cycle.
In 2026, harm reduction and health monitoring have become a much bigger part of the bodybuilding conversation. Regular bloodwork is now considered standard practice among experienced users, with many closely tracking markers such as hematocrit, AST and ALT liver enzymes, ApoB, HDL, LDL, estradiol, fasting glucose, kidney function, and blood pressure throughout a cycle.
Designing the Best Testosterone Cycles
Designing a testosterone cycle involves far more than simply choosing a weekly dosage. In 2026, cycle planning has become increasingly focused on long-term health management, recovery, and maintaining stable hormone levels alongside muscle growth and performance enhancement.
Choosing the Testosterone Ester
The first step is selecting the testosterone ester. Short esters like Testosterone Propionate clear the system quickly and require more frequent injections, while longer esters such as Testosterone Enanthate and Testosterone Cypionate provide more stable blood levels with fewer injections per week. Sustanon remains popular for users who prefer a blend of both short and long esters.
The ester choice often depends on the goal of the cycle. Propionate is commonly used during cutting phases and contest prep, while Enanthate and Cypionate are typically favored during offseason muscle-building phases or TRT protocols.
Running Testosterone Solo vs Stacking Compounds
The second major decision is whether testosterone will be used as a standalone compound or combined with additional anabolic agents.
Beginner users often start with testosterone-only cycles to better understand how their body responds to estrogen conversion, androgenic effects, and hormonal suppression. More advanced users may stack testosterone with compounds such as Nandrolone Phenylpropionate (NPP), Equipoise, Primobolan, or Masteron depending on whether the goal is mass gaining, recomposition, or contest preparation.
Each added compound introduces additional variables and potential side effects, making cycle complexity significantly higher.
Continued Health Management
Modern testosterone cycle design places far greater emphasis on health monitoring than in previous decades. Experienced users now commonly prioritize longevity markers and cardiovascular health alongside physique goals.
PCT for Testosterone
Whenever you use outside hormones like testosterone or other anabolic steroids, your body naturally adjusts by dialing down its own production. It’s basically your endocrine system saying, “we’ve got enough coming in, so we’ll take a break.” This happens through a normal feedback loop, and unfortunately, it’s something you can’t avoid with steroid use.
Because of that, once a cycle ends, it’s common to see your natural testosterone levels drop. Along with that, hormones like LH (luteinizing hormone) and FSH (follicle-stimulating hormone) also tend to stay suppressed for a while. These two play a key role in signaling your body to produce testosterone in the first place, so when they’re low, your natural production slows down.
That’s where post-cycle therapy (PCT) comes in. The goal is to help your body gradually restart its own testosterone production while also keeping estrogen in check as things rebalance.
A typical PCT approach may include:
- A SERM (Selective Estrogen Receptor Modulator) to help stimulate natural testosterone signaling
- HCG (human chorionic gonadotropin) to help “wake up” the testes and support production during recovery
- In some cases, HMG (human menopausal gonadotropin) and L-carnitine are also used as additional support
The overall idea is pretty simple: you’re helping your body transition back to running on its own again after being externally supported.
Conclusion
Testosterone remains the backbone of bodybuilding cycles for one simple reason: it consistently delivers results.
Whether the goal is lean muscle growth, offseason size, strength progression, or physique preservation during a cut, testosterone continues to be one of the most reliable anabolic compounds available.
But the conversation around testosterone use in 2026 has evolved. Bigger no longer automatically means better. More users now prioritize longevity markers, bloodwork, cardiovascular health, and recovery instead of blindly pushing dosage higher.
Used recklessly, testosterone can create serious health complications. Used intelligently, monitored carefully, and paired with disciplined training and nutrition, it remains one of the most effective performance-enhancing compounds in bodybuilding.
FAQs
What is the best testosterone cycle for beginners?
Most beginners start with a testosterone-only cycle using Enanthate or Cypionate at moderate weekly doses. Simpler cycles make it easier to assess side effects and hormone response.
How long should a testosterone cycle last?
Most testosterone cycles last between 10 and 16 weeks depending on the ester, dosage, and overall goal.
Is testosterone safer than other steroids?
Testosterone is generally considered more predictable than harsher anabolic steroids, but it still carries cardiovascular, hormonal, and androgenic risks.
Do testosterone cycles require PCT?
In most cases, yes. Exogenous testosterone suppresses natural hormone production, and recovery protocols are commonly used after cycles.
Can you run testosterone without stacking other compounds?
Yes! Testosterone-only cycles remain one of the most common approaches, especially for beginners who want to understand how their body responds before introducing additional compoundsl