
Before undergoing testosterone replacement therapy (TRT), it is important to understand the physiology of testosterone, who should get TRT, and the different formulations of TRT such as injections, gels, and creams.
We’ve put together this article explaining the pros and cons of two of the most common formulations of TRT – Injections and gels – to help you be well-informed before making the decision with your doctor when it comes to choosing the best formulation of TRT – Testosterone Gel vs Injection.
Key Takeaways
- Each TRT formulation has its own pros and cons.
- You need to discuss with your doctors the best formulation that fits you the most. What works for you doesn’t necessarly work for others.
- Both injectable and topical (gel) testosterone formulations show efficiency in improving psychosexual functions.
- Testosterone Enanthate is the cheapest among all testosterone injections.
- NTGs may have the potential to be a suitable TRT option in men desiring fertility.
Testosterone Hormone
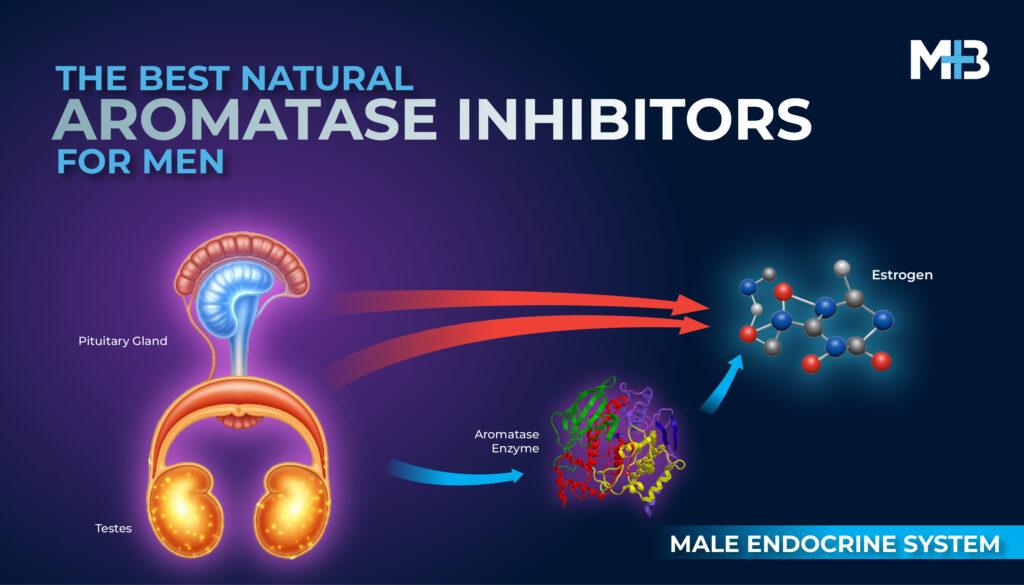
Testosterone is an essential, vital sex hormone for males, required for differentiation, developmental growth, and phenotype maintenance. [1]
Testosterone is currently approved by the Food and Drug Administration (FDA) for primary or secondary hypogonadism.
With the worldwide increase in men’s life expectancy and the development of proper testosterone preparations, the interest in prescribing TRT has dramatically increased.
In young, healthy men (20 – 30 years old), the normal levels of serum testosterone (400 – 700 ng/dL) are controlled by the hypothalamic-pituitary-gonadal axis and are maintained within the normal range of 300–800 ng/dL. [1]
Serum testosterone levels decline gradually with age in men after the third decade of life at an approximate rate of 1-2% per year, varying from one to another, and are affected by several factors such as adiposity and chronic diseases. [1]
Who Needs TRT?!
Hypogonadism in men is the clinical syndrome that results from failure of the testis to produce adequate levels of testosterone and sperm cells. [2]
Classical hypogonadism resulting in markedly reduced T levels due to identifiable congenital or acquired disorders at the testicular (primary hypogonadism), hypothalamic-pituitary (secondary hypogonadism) or combined levels is universally accepted indication for testosterone replacement therapy. [3]
In 2018, the American Urological Association recommended the use of TRT in patients with total testosterone < 300 ng/dl. [4]
How Do You Know That You Have Testosterone Deficiency?
Here is a list of the most common symptoms and signs of testosterone deficiency:
- Anemia.
- Depressed mood.
- Erectile dysfunction.
- Decreased libido and sexual desire.
- Reduced muscle mass and strength.
- Reduced bone mass and osteoporosis.
- Insomnia and a reduced sense of general well-being.
- Forgetfulness, difficulty in concentration, and loss of memory.
What Is Next? Go See A Doctor!
Your lab results returned, and your total testosterone was < 300 ng/dl. What’s next? Now, schedule your appointment with specialist.
Your doctor will review your medical history and tailor a treatment plan that fits your clinical presentation.
Testosterone Replacement Therapy
Several testosterone preparations and modes of application are available of which those producing physiologic serum levels should be preferred e.g. preferentially transdermal gels and long-acting intramuscular testosterone undecanoate. [3]
Testosterone Injections
Long-acting Intramuscular Testosterone
Long-acting intramuscular (IM) injections of T esters, such as T enanthate, T cypionate and a mixture of esters have been used for many years for the treatment of hypogonadism.
Testosterone Enanthate
Testosterone enanthate has been the most common preparation for testosterone substitution since its introduction in the early 1950s. [5]
It has a terminal half-life of 4.5 days. Its maximum concentrations are reached after 10 h following a single injection of 250 mg. [5]
Multiple-dose pharmacokinetics reveal an optimal injection interval of 2-3 weeks at a dose of 200-250 mg. [5]

- The main advantages of these formulations, especially T enanthate, are the effectiveness in initiating and
- Freedom from daily administration.
- The need for deep IM injection every 1–3 weeks.
- Fluctuations in serum T levels resulting in fluctuations in energy, mood and libido in many patients. These fluctuations are more pronounced when dosing interval is increased.
Testosterone Enanthate
Testosterone Cypionate and Testosterone Cyclohexanecarboxylate
Testosterone cypionate and testosterone cyclohexanecarboxylate resemble the pharmacokinetic properties of testosterone enanthate. [5]
They do not provide an advantage over the enanthate ester.
Testosterone Propionate
Testosterone propionate has a terminal half-life of only 19 h. After a single injection of 50 mg, maximum concentration is reached after 14 h. It requires frequent injection. [5]
Multiple-dose pharmacokinetics reveal optimal intervals of 2-3 days, but fluctuations below normal-range values persist. Therefore, it is not suitable for long-term treatment of hypogonadism. [5]
Testosterone Undecanoate
An extra long-acting injectable form of testosterone undecanoate in castor oil, with even longer half-life of about 34 days, that allows increased dosing intervals of up to three months.
It needs to be administered with an initial dose of 750 mg, followed 4 weeks later by another 750 mg dose. This is then followed by an intramuscular injection once every 10 weeks.
Individual intervals are determined according to serum testosterone levels which are measured immediately before the next injection.
Values that are too high lead to extension of injection intervals, those that are too low to a shortening in injection intervals.
Slow intragluteal injections are recommended.
Adverse Effects of Injectable Testosterone
Cardiovascular Events
In a retrospective analysis of three databases, use of injectable preparations was associated with a greater risk of MI and stroke when compared with T gel use.
Erythrocytosis
Erythrocytosis is a common adverse effect of T administration, particularly with T ester injections and in older men. Erythrocytosis also occurred significantly earlier in men on injectable T formulations when compared with the other two formulations.
Pulmonary oil Microembolism (POME)
Although the injectable preparations are generally considered very safe, there is a risk of pulmonary oil microembolism (POME).
It’s clinically characterized by brief respiratory symptoms such as cough, urge to cough and dyspnea immediately after the injection.
It has been observed after injection of testosterone enanthate in castor oil at a rate of 1.5% of injections. Similarly, it may occur after intramuscular injection of testosterone undecanoate, although at a much lower rate.
The FDA has required a special warning of POME when licensing intramuscular testosterone undecanoate (Aveed®) in the USA. This preparation contains only 750 mg testosterone undecanoate and therefore requires slightly shorter injection intervals of about 10 weeks. [6]
Monitoring
Injectable testosterone enanthate or cypionate: measure serum testosterone level midway between injections. If testosterone is 700 ng/dl (24.5 nmol/liter) or 400 ng/dl (14.1 nmol/liter), adjust dose or frequency. [1]
Injectable testosterone undecanoate: measure serum testosterone level just prior to each subsequent injection and adjust the dosing interval to maintain serum testosterone in mid-normal range.
Transdermal Testosterone Gel
A further transdermal application is the use of testosterone gels applied to large skin areas in order to allow sufficient amounts of the hormone to be resorbed.
Where To Apply T Gel? and When?
Physiological levels result when these gels, applied in the morning to the upper arm, shoulders and abdomen are left to dry for five to ten minutes.
Advantages
Stable T Serum Levels
Transdermal Testosterone gels result in relatively stable Testosterone serum levels and their pharmacokinetic profile mimics the physiological diurnal variations of T concentration.
Serum testosterone levels are maintained when the application site is washed 4–6 h after application of the testosterone gel.
Easy and Fast To Eliminate
Due to their short duration of action, the effect of TRT can be quickly eliminated upon removal should an adverse effect occurs.
These advantages make the transdermal preparations the preferred treatment modality especially when initiating therapy, for older men with hypogonadism or for patients with fluctuating symptoms caused by other formulations.
Lean Body Mass
In his 3-year clinical trial, Storer et al. confirmed the effects of testosterone replacement therapy, using 7.5 g of 1% testosterone gel, on lean body mass in 135 community-dwelling older men over 60 years of age with baseline total testosterone levels of 100–400 ng/dL and free testosterone of <50 pg/mL. [7]
Bone Mineral Density
The latest study by Snyder et al., reported that 12-months’ treatment with 5 g/day of 1% testosterone gel in 110 men over 65 years of age and serum testosterone levels below 275 ng/dL resulted in a significant increase in volumetric bone mineral density. [8]
Sexual Activity
Similarly, 1-year replacement therapy with 5 g/day of 1% testosterone gel in 234 older men with low libido and average serum testosterone levels below 275 ng/dL has also significantly improved 10 of 12 measures of sexual activity assessed using the Psychosexual Daily Questionnaire. [9, 10]
Disadvantages
Obesity
In some hypogonadal men, normal serum T levels cannot be achieved. Especially, patients with high BMI may require higher doses, since obesity seems to affect the pharmacokinetics of transdermal preparations.
Avoiding Unintended Testosterone Gel Transfer
The risk of unintentionally transferring testosterone gel through skin contact is significant, particularly for women and children.
Direct skin contact with others after applying testosterone gels can lead to androgenization in women, girls, and boys. Reports of such cases prompted the FDA in 2011 to mandate a black box warning for testosterone gel packaging, highlighting the seriousness of this risk.
To minimize the chances of transfer, follow these precautions:
- Wash hands thoroughly after applying the gel.
- Avoid direct skin contact with others until the gel has fully dried.
- Cover the application site with clothing to prevent accidental exposure.
By following these steps, you can safely use testosterone gels while protecting those around you.
Other disadvantages include:
- The need for daily administration.
- Relatively high cost.
Nasal Testosterone Gel

The recently approved nasal T gel represents a novel non-invasive route for TRT.
It is seen to be advantageous over topical gels because of the easy of use and the lower risk of transference.
It comes with the disadvantages of thrice daily application, intolerance by men with underlying nasal or sinus pathology and paucity of data regarding overall efficacy and safety.
With regards to fertility, Conners et al found that 4.5% NTG two or three times a day restored serum testosterone levels while only decreasing gonadotropin levels minimally, keeping serum FSH and LH values within the normal range.
Its short half-life results in a return of serum testosterone to near baseline levels between doses. It is theorized that this decreases its effect on the pulsatile release of GnRH by the hypothalamus.
Based on what is found by future studies, NTGs may have the potential to be a suitable TRT option in men desiring fertility.
Serum T concentrations vary substantially when a gel is used but not in a predictable way. Therefore, two T measurements should be done before making dose adjustments.
Monitoring
Adjust dose to achieve serum testosterone level in the mid-normal range.
Testosterone substitution must be monitored at regular intervals, best at 3, 6 and 12 months after initiation and then annually.
Patients on topical gels, patches, and intranasal formulations should have their testosterone checked between 2 to 4 weeks after commencement of therapy.
Prescribtion, Compliance and Market Size
Survey data including prescribers from North America, Europe, Oceana, Latin America, and Caribbean demonstrate stronger physician preference in the USA for gel-based TRT over injectable variants, with 67.7% in North America preferring gel.
The preference in the USA is reflected in studies on prescription patterns demonstrating 44.6–67.8% of TRT as gel-based therapies.
A study on almost 11 million prescriptions from 2001 to 2011 indicated a five-fold increase in gel use compared with a three-fold increase in overall TRT.
In a study evaluating 15 952 patients, after 3 mo of initiating TRT, 52% of patients continued topical and 31% continued injection therapies. At 1 yr in this same cohort, 18% continued topical and 5% continued injection therapies.
Another study evaluating only gels reported overall compliance of 34.7% and 15.4% at 6 mo and 1 yr, respectively, with no statistical difference between gel brands.
Final Thoughts
There’s no universal solution for Testosterone Replacement Therapy (TRT). Both injections and gels effectively address low testosterone symptoms in different ways.
The best choice depends on your unique needs and lifestyle. That’s why it’s crucial to fully understand each method’s pros and cons.
Being informed empowers you to make confident decisions about your treatment. Talk to your healthcare provider about your options.











if I do a combination of gel and shots doing one every two weeks followed by the other for two weeks?